How Doctors Diagnose Skin Rashes: Tests, Exams, and Medical Evaluation Guide

Diagnosing a skin rash is one of medicine's most nuanced challenges. Unlike most conditions where a blood test or imaging study delivers a clear answer, the skin tells its story through subtle visual and tactile clues — clues that require trained clinical interpretation, systematic investigation, and sometimes laboratory confirmation before a definitive diagnosis can be made.
The complexity of rash diagnosis arises from several realities simultaneously at work. First, the skin expresses a vast range of conditions — over 3,000 distinct dermatological conditions are recognized — yet many of them look remarkably similar, particularly in early stages or on diverse skin tones. Second, the same underlying condition can look dramatically different depending on its stage of evolution, the anatomical location involved, and the individual's immune status. Third, rashes can be the presenting sign of systemic diseases — lupus, vasculitis, endocarditis, lymphoma — where the skin manifestation is downstream of a deeper pathological process.
Accurate diagnosis requires integrating four streams of information: the patient's medical history, the physical characteristics of the rash itself, targeted laboratory or procedural investigations, and differential diagnosis reasoning that systematically considers and excludes competing diagnoses. This guide walks through each of these steps in detail, explaining what physicians are looking for, why specific tests are ordered, and how results guide treatment decisions.
Understanding this diagnostic process empowers you to participate more effectively in your medical care — to provide the right information to your physician, to understand why certain tests have been recommended, and to recognize when your rash requires urgent rather than routine evaluation.
Medical History Review in Rash Diagnosis
Before examining the skin, a thorough medical history is the foundation of every rash diagnosis. Studies show that in dermatology, the medical history alone leads to the correct diagnosis in over 60% of cases — more than any single physical finding or laboratory test. Physicians use structured history-taking to narrow the differential diagnosis and guide which physical findings to prioritize.
Symptom Timeline
When did the rash first appear? Did it start at one site and spread? How rapidly did it evolve? Is it constant or intermittent? Acute onset within hours suggests urticaria or anaphylaxis; gradual onset over days suggests contact dermatitis or viral exanthem; a waxing and waning course over months suggests eczema or psoriasis. The timeline is often the first filter in diagnosis.
Exposure Tracking
What has the patient been exposed to in the 72 hours before the rash? New soaps, detergents, cosmetics, or lotions? New clothing or fabrics? Contact with plants, animals, or latex? Occupational chemical exposures? Contact allergens typically produce a rash 24–72 hours after exposure (delayed hypersensitivity), while immediate allergic reactions (IgE-mediated) occur within minutes to an hour.
Medication History
Any medication — prescription, over-the-counter, herbal, or supplement — started in the 6 weeks prior to rash onset is a potential culprit. The most common drug rash triggers include antibiotics (amoxicillin, sulfonamides), NSAIDs, anticonvulsants, and allopurinol. Drug rashes can appear weeks after starting a medication, making the connection easy to miss without systematic questioning.
Travel History
Recent international travel opens the differential to geographic pathogens: dengue fever (blanching rash with thrombocytopenia), Zika virus, rickettsial diseases, leishmaniasis, and cutaneous larva migrans. Even domestic travel (camping, swimming in lakes) raises the risk of Lyme disease, Rocky Mountain spotted fever, and swimmer's itch.
Allergy History
Known allergies to foods, medications, or environmental allergens inform the diagnosis of allergic rashes. A personal or family history of atopy (eczema, asthma, allergic rhinitis) significantly raises the probability of atopic dermatitis. Previous reactions to specific products or chemicals identifies likely contact allergen suspects before patch testing.
Family Skin Disease History
Many skin conditions have a significant hereditary component. Psoriasis has about 30% heritability — a first-degree relative with psoriasis increases risk three-fold. Atopic dermatitis, ichthyosis, and epidermolysis bullosa have strong genetic associations. Family history of autoimmune conditions (lupus, rheumatoid arthritis) raises suspicion for immune-mediated rashes in the patient.
Physical Examination of Skin Rashes
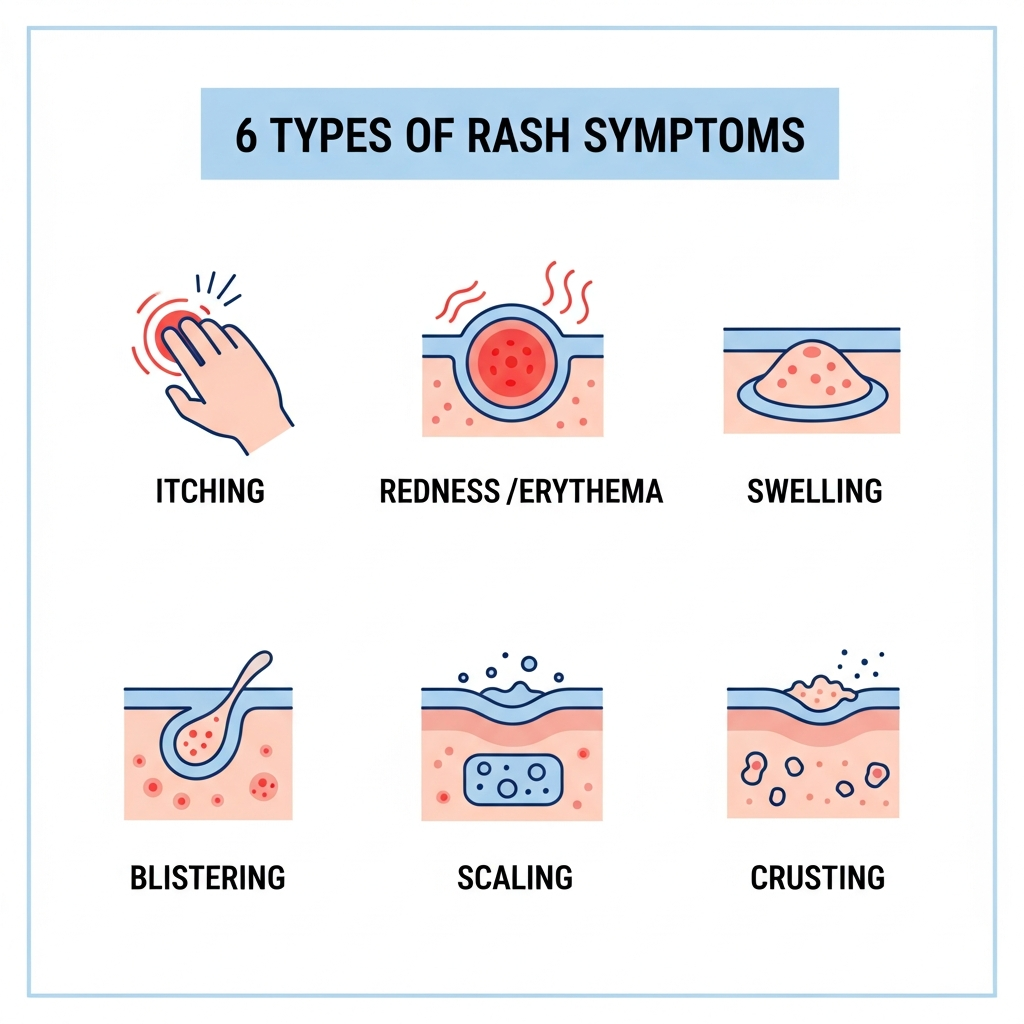
The physical examination of a rash is highly systematic. Dermatologists use precise descriptive language — developed over centuries of clinical observation — to characterize lesions in a way that allows findings to be communicated consistently between physicians and to guide diagnosis. The six dimensions of rash examination are:
Rash Color Interpretation
Color carries major diagnostic weight. Bright red indicates acute inflammation (cellulitis, contact dermatitis, sunburn). Salmon-pink suggests psoriasis. Violaceous (purple-red) hue is characteristic of lichen planus and dermatomyositis. Silver-white scale on a red base is nearly pathognomonic for psoriasis. Non-blanching red-to-purple color (petechiae, purpura) indicates blood vessel leakage — potentially serious. On darker skin tones, erythema may appear as hyperpigmented brown or gray patches rather than red, requiring trained observation.
Rash Border Patterns
A well-demarcated (sharp) border strongly suggests psoriasis or contact dermatitis following an exact exposure area. Poorly demarcated (diffuse, blending) borders are typical of eczema and cellulitis. An annular (ring-shaped) border with a clear center is characteristic of ringworm, granuloma annulare, or erythema migrans (Lyme). Serpiginous (snake-like, winding) borders occur in cutaneous larva migrans. The Koebner phenomenon (new lesions appearing along scratch lines) is characteristic of psoriasis and lichen planus.
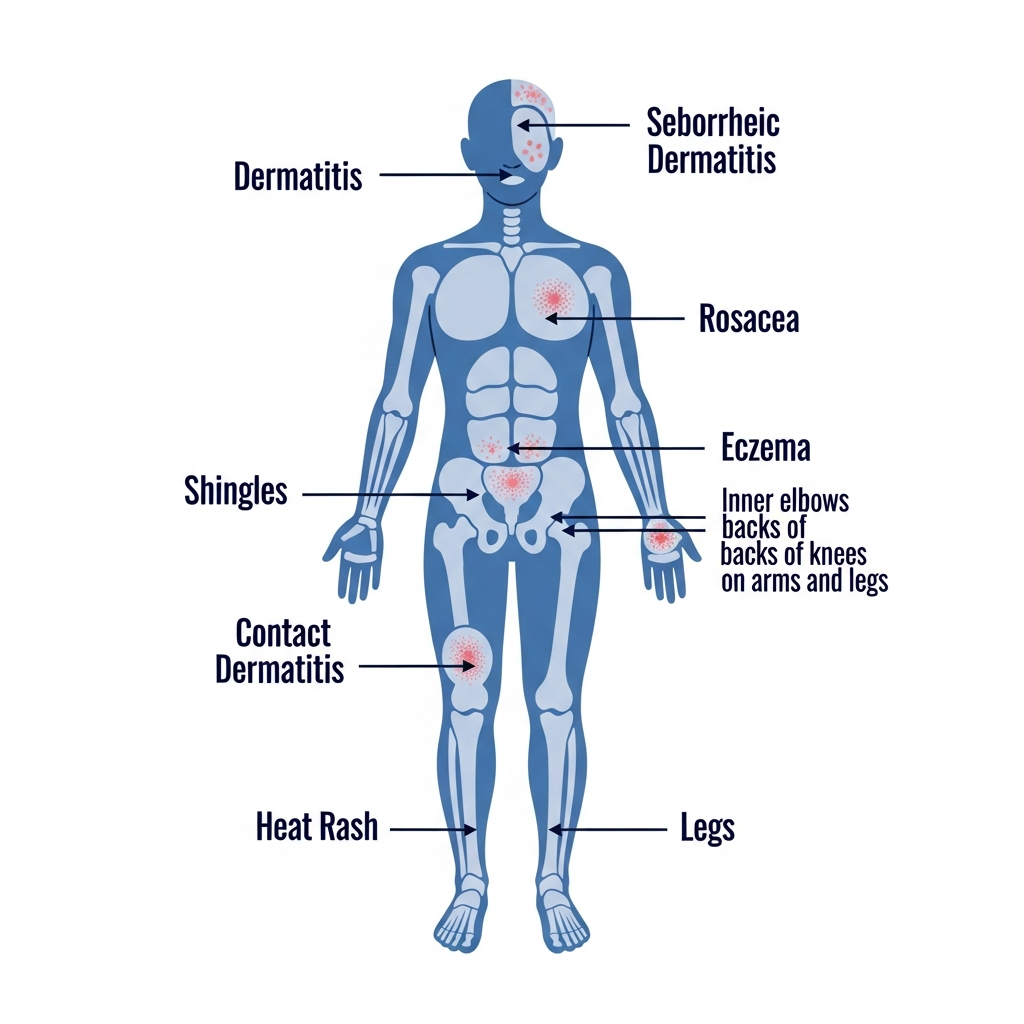
Distribution Patterns
Where the rash appears on the body is one of the most powerful diagnostic signals. Flexural distribution (elbow creases, knee creases) strongly favors eczema. Extensor distribution (outside of elbows and knees) favors psoriasis. Photo-distributed rash (face, V-neck, forearms) suggests photosensitivity from lupus, porphyria, or drug reactions. A dermatomal (unilateral, following a nerve root) distribution is pathognomonic for shingles. Glove-and-stocking distribution suggests erythromelalgia or peripheral vascular disease. Symmetric bilateral rash on the face (butterfly pattern) is a lupus hallmark.
Texture and Scaling
Texture reveals histological information before any biopsy is done. Sandpaper texture in scarlet fever reflects superficial papules. Silvery, adherent scale on psoriasis indicates rapid cellular turnover. Greasy yellow scale in seborrheic areas points to seborrheic dermatitis. Lichenification (skin thickening with accentuated skin lines) results from chronic rubbing and is the hallmark of chronic eczema. Dermoscopy magnifies texture to reveal follicular plugging (lupus), Wickham's striae (lichen planus), and strawberry pattern vessels (rosacea).
Swelling Indicators
Swelling within a rash indicates fluid accumulation or deeper tissue involvement. Raised, dome-shaped urticarial wheals that pit and disappear within 24 hours are hives. Tense, large bullae (blisters) suggest bullous pemphigoid or second-degree burns. Pitting edema alongside a rash may indicate venous stasis or lymphedema. Non-pitting, board-like swelling in a spreading rash suggests necrotizing fasciitis — a surgical emergency. Soft, fluctuant swelling indicates a fluid collection (abscess).
Lymph Node Checks
Palpating regional lymph nodes — the lymph nodes that drain the area of the rash — is a standard part of the skin examination. Enlarged, tender lymph nodes alongside a skin rash suggest active infection or drug hypersensitivity syndrome (DRESS). Enlarged, firm, non-tender nodes in a patient with chronic skin changes raise concern for lymphoma (cutaneous T-cell lymphoma / mycosis fungoides). Widespread lymphadenopathy alongside a rash is characteristic of secondary syphilis, mononucleosis, and systemic drug reactions.
Common Diagnostic Tests for Skin Rashes
Targeted laboratory and procedural tests extend the diagnostic reach beyond clinical examination. The key is appropriate test selection — ordering the right test based on the clinical hypothesis, not a blanket panel for every patient.
Skin Scraping Test
Low RiskPurpose
Identifies fungal infections (dermatophytes, yeasts) and parasites such as scabies mites by collecting cells and debris from the skin surface for microscopic examination.
When Used
Ordered when a ring-shaped, scaly, or moccasin-pattern rash suggests tinea, or when intense nocturnal itch in characteristic locations (web spaces, wrists, genitalia) raises suspicion for scabies.
What Results Show
A potassium hydroxide (KOH) preparation dissolves skin cells and reveals fungal hyphae (long branching filaments) under the microscope if a fungal infection is present. Scabies mites, eggs, or fecal pellets (scybala) confirm infestation. A negative result doesn't rule out fungal infection if sampling was suboptimal.
Patch Allergy Testing
Low RiskPurpose
Identifies specific contact allergens responsible for allergic contact dermatitis — the most accurate way to determine which substances are triggering a patient's chronic or recurrent eczema-like rash.
When Used
Recommended when contact dermatitis is suspected (rash in a location or pattern consistent with allergen contact), when eczema is not responding to standard treatment, or before introducing new skin care or cosmetic products.
What Results Show
Small quantities of standardized allergen panels are applied to the back under adhesive tape for 48 hours, then read at 48 and 96 hours. A positive result (redness, induration, vesicles at the test site) identifies the specific allergen. The European Baseline Series covers the 30+ most common contact allergens.
Blood Tests for Rash Diagnosis
Low RiskPurpose
Blood tests help identify systemic causes of rash — including autoimmune conditions, infections, drug reactions, and organ dysfunction — as well as guide treatment decisions for chronic inflammatory skin diseases.
When Used
Ordered when systemic disease is suspected (e.g., lupus, vasculitis, psoriatic arthritis), when rash accompanies fever or lymphadenopathy, before starting immunosuppressive therapy, or when allergy-specific IgE levels are needed for suspected atopic disease.
What Results Show
Key panels include: Complete blood count (CBC) — identifies eosinophilia (elevated in allergic/parasitic conditions), elevated white blood cells (infection); Inflammatory markers (ESR, CRP) — elevated in active inflammatory or autoimmune disease; ANA panel — screens for lupus and connective tissue diseases; Total IgE and specific IgE (RAST) — identifies allergic sensitization; Liver and kidney function tests — detect systemic disease; Serological tests for Lyme disease, syphilis, or specific viral infections.
Bacterial Culture
Low RiskPurpose
Identifies the specific bacteria causing a skin infection and determines antibiotic susceptibility — critical for selecting effective treatment, especially when MRSA (methicillin-resistant Staphylococcus aureus) is possible.
When Used
Used when a bacterial infection is suspected (impetigo, cellulitis, abscess, infected eczema) but initial antibiotic treatment has failed, when the infection appears unusually aggressive, or in immunocompromised patients where antibiotic resistance is a concern.
What Results Show
A swab from the wound or blister fluid, or a skin biopsy sample, is placed on growth media and incubated for 24–72 hours. The laboratory identifies the organism (e.g., Staphylococcus aureus, Streptococcus pyogenes) and tests its sensitivity to a panel of antibiotics, guiding targeted therapy.
Viral Testing
Low RiskPurpose
Identifies the specific virus responsible for a viral rash — important for contagion management, antiviral treatment decisions, and assessment of complications, particularly in immunocompromised patients.
When Used
Ordered when herpes simplex, varicella-zoster (chickenpox or shingles), or Epstein-Barr virus (mononucleosis) is suspected; when a rash erupts after travel; or in atypical presentations where viral cause needs confirmation.
What Results Show
Viral testing methods include: Tzanck smear — a rapid bedside test showing multinucleated giant cells in herpes simplex or varicella infections; PCR (polymerase chain reaction) — the gold standard for detecting viral DNA/RNA from lesion swabs or blood; Serology (IgM/IgG antibodies) — identifies prior exposure and current active infection; Direct fluorescent antibody (DFA) testing — rapid identification of herpes viruses from vesicle scraping.
Fungal Microscopy and Culture
Low RiskPurpose
Definitively confirms fungal infections when clinical appearance is insufficient, guides antifungal selection, and identifies the specific fungal species — particularly important for nail infections (onychomycosis) and scalp ringworm (tinea capitis).
When Used
Used for suspected nail fungal infection before prescribing systemic antifungals; atypical or treatment-resistant tinea; scalp infections in children; or when pityriasis versicolor needs confirmation via Wood's lamp or microscopy.
What Results Show
KOH preparation of scale, nail clippings, or hair stubs reveals fungal elements under the microscope within 30–60 minutes. Fungal culture on Sabouraud dextrose agar grows colonies over 2–4 weeks, allowing species identification. Wood's lamp examination causes certain fungi (tinea capitis from Microsporum species) to fluoresce green under UV light — a rapid, non-invasive screening tool.
Skin Biopsy
Low–Moderate RiskPurpose
Provides a definitive histopathological diagnosis for rashes that cannot be identified through clinical examination or simpler tests alone. It is the gold standard for diagnosing inflammatory, autoimmune, and neoplastic skin conditions.
When Used
Recommended for rashes that are persistent and unresponsive to treatment, have an atypical appearance, are suspected to represent an autoimmune blistering condition, vasculitis, or skin lymphoma, or when melanoma or other skin cancer must be excluded.
What Results Show
A small sample of skin (typically 3–4mm diameter via punch biopsy, or an elliptical excision) is taken under local anesthetic and sent to a dermatopathologist. H&E staining shows the cellular architecture; special stains (PAS for fungi, Gram stain for bacteria) and immunofluorescence (for autoimmune blistering diseases) may be added. Results typically return in 7–14 days. The pathology report identifies the specific inflammatory pattern, infectious organism, or tumor type.
Differential Diagnosis Approach
Differential diagnosis is the systematic process of distinguishing between conditions that share similar features. In dermatology, this involves constructing a ranked list of possible diagnoses based on the history and examination, then using targeted tests to confirm one and exclude the others. Below are four of the most clinically important rash differential pairs:
| Diagnostic Pair | First Condition | Second Condition | Key Distinguishing Test |
|---|---|---|---|
| Fungal vs Allergic Rash | Ring-shaped border, KOH positive, responds to antifungal | No ring shape, KOH negative, responds to antihistamine/steroid | KOH skin scraping + patch testing |
| Viral vs Autoimmune Rash | Blood tests: ANA panel + viral serology | ||
| Bacterial vs Parasitic Rash | Culture + skin scraping for mites | ||
| Eczema vs Psoriasis | Clinical distribution + biopsy if uncertain |
When Immediate Medical Evaluation Is Needed
While most rashes can be evaluated at a scheduled appointment, certain combinations of symptoms require emergency evaluation without delay. The following presentations should be treated as medical emergencies:
Rapidly Spreading Rash
A rash expanding its borders over hours — especially if warm and tender — may indicate aggressive cellulitis, necrotizing fasciitis, or a spreading drug reaction. Mark the border and monitor: expansion over 2 hours is an emergency.
Purple or Black Non-Blanching Rash
Petechiae or purpura that do not blanch under glass-pressure may indicate meningococcemia, thrombocytopenia, or vasculitis. This is a potential life-threatening emergency — call 999/911 immediately.
Rash with High Fever
A rash with fever above 39°C (102°F) suggests a serious systemic infection (scarlet fever, Rocky Mountain spotted fever, sepsis) or drug hypersensitivity syndrome (DRESS). Requires urgent same-day evaluation.
Rash with Breathing Problems
Respiratory compromise alongside a rash indicates anaphylaxis. Epinephrine is the first-line treatment — antihistamines alone are insufficient. Call emergency services immediately.
Rash with Severe Pain
Pain disproportionate to visible skin findings, or rapidly worsening pain beneath a rash, may indicate necrotizing fasciitis — a rapidly progressing, life-threatening deep tissue infection requiring emergency surgery.
Telehealth Rash Diagnosis
Photo Diagnosis Limitations
Teledermatology via photograph cannot replicate tactile assessment (texture, firmness, temperature), dermoscopy, or the dynamic observation of a rash evolving over minutes in the clinic. Image quality, lighting, and skin tone all affect diagnostic accuracy. Studies suggest photo-based diagnosis has 70–80% concordance with in-person diagnosis for common conditions — better for distinctive rashes (psoriasis, ringworm) and less reliable for ambiguous presentations.
Symptom Questionnaires
Structured symptom questionnaires used in teledermatology platforms gather the same history a physician would take in person: symptom duration, location, associated symptoms, medications, exposures, and prior treatments. Combined with clear photographs from multiple angles and lighting conditions, these questionnaires significantly improve remote diagnostic accuracy and help identify patients who require in-person evaluation.
When Telemedicine Is Useful
Teledermatology is most useful for: initial assessment of mild-to-moderate non-emergency rashes; follow-up monitoring of known chronic conditions (eczema, psoriasis) between appointments; prescription refills for established diagnoses; triaging which patients need urgent in-person evaluation; and serving patients in areas with limited dermatology access. It is not appropriate for suspected infections requiring culture, autoimmune blistering diseases, or any emergency presentation.
Rash Diagnosis Timeline
Acute Rash Evaluation (Days 1–7)
Initial presentation: history, physical exam, clinical diagnosis or initial tests ordered (KOH, culture swab, blood draw)
Rapid test results return: bacterial culture preliminary, blood CBC/CRP, viral serology for common viruses
Treatment response assessment: rash improving confirms diagnosis; no improvement prompts re-evaluation and additional testing
Biopsy results return if ordered; fungal culture results; patch test reading for contact allergens
Chronic Rash Evaluation (Weeks to Months)
Biopsy results, complete patch test read at 96h, full autoimmune panel results; refine working diagnosis
Treatment trial: assess response to topical steroids, antifungals, or antihistamines depending on working diagnosis
Follow-up appointment to confirm treatment response, adjust treatment, monitor for recurrence or complications
Chronic conditions (eczema, psoriasis) require ongoing monitoring of disease activity, treatment side effects, and quality of life impact
Frequently Asked Questions
Expert answers to the most common questions about rash diagnosis.
Explore Rash Causes and Treatments
Medical Disclaimer: The diagnostic information, test descriptions, and clinical guidance on this page are for educational purposes only and do not constitute medical advice, diagnosis, or treatment recommendations. Rash diagnosis requires in-person clinical evaluation by a qualified healthcare professional. Do not delay seeking medical care based on information found on this page. In a medical emergency involving a skin rash, call your local emergency services immediately. Read our full medical disclaimer.