Common Skin Rash Pictures: Visual Guide to Identifying Rash Types
Visual identification of skin rashes is one of the most challenging — and most important — skills in both clinical medicine and patient self-education. The skin is the body's largest organ and a window into systemic health: rashes can represent simple irritation, contagious infections, autoimmune conditions, or — in rare cases — life-threatening emergencies.
This comprehensive visual guide provides medically accurate descriptions and educational illustrations for eight major categories of skin rashes: eczema, psoriasis, viral rashes, fungal infections, allergic rashes, heat rash, bacterial rashes, and parasitic infestations. Each section includes detailed descriptions of visual characteristics, distinguishing features, symptom checklists, and guidance on when to seek medical care.
It is important to understand that while photographic references significantly improve rash literacy and help patients communicate with their healthcare providers, they cannot replace professional clinical evaluation. Rash presentation varies across skin tones, stages of evolution, individual immune responses, and concurrent conditions. A dermatologist has access to dermoscopy, skin biopsy, patch testing, and laboratory analysis that extend far beyond what photographic comparison can offer.
Use this guide to educate yourself, identify warning signs that require urgent care, prepare for a medical appointment, and understand the spectrum of what each rash type can look like. The goal is to make you a more informed patient — not to replace the physician-patient relationship.
Eczema Rash Pictures

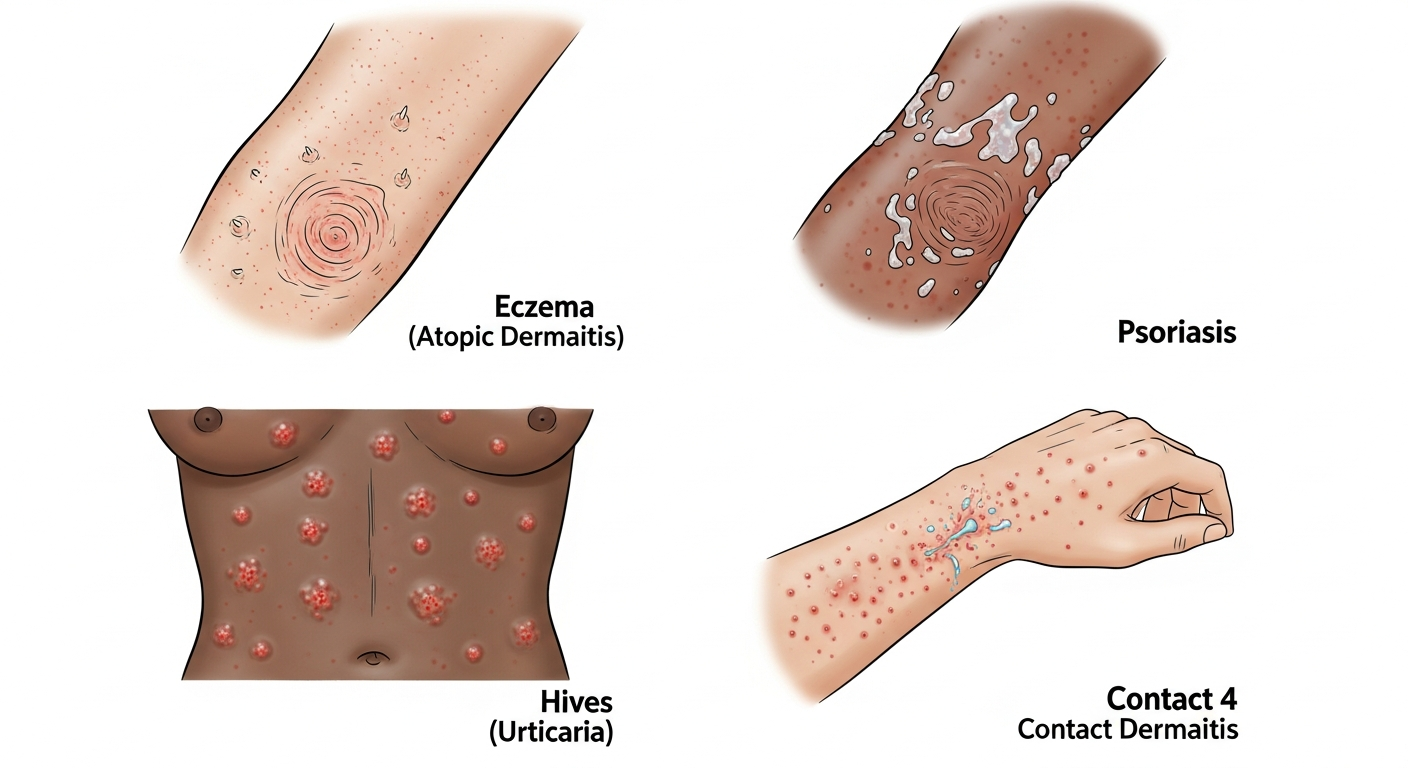
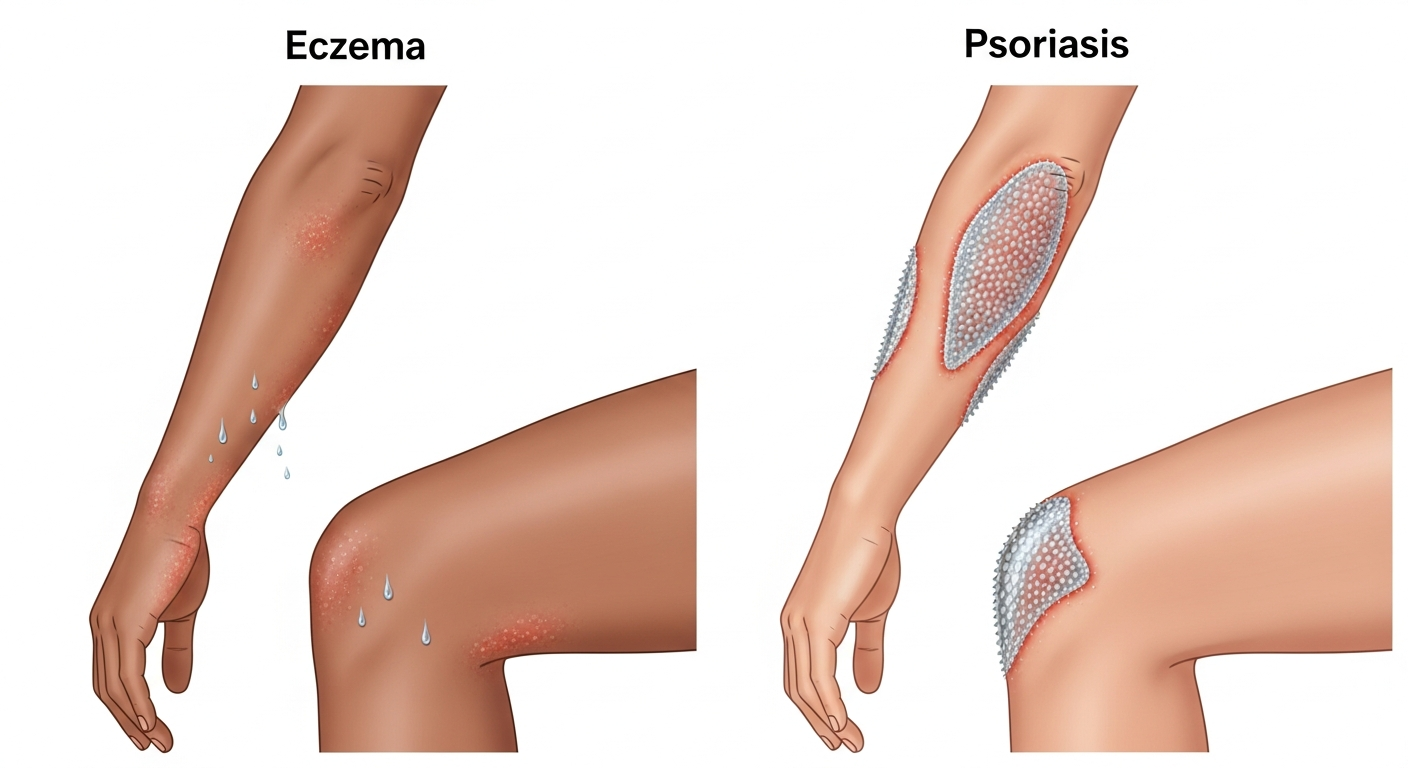
Eczema, also known as atopic dermatitis, is one of the most prevalent chronic inflammatory skin conditions worldwide, affecting an estimated 15–20% of children and 1–3% of adults at some point during their lives. The visual presentation of eczema is highly variable, making photographic reference guides particularly valuable for self-education and early identification. In most cases, eczema appears as patches of intensely itchy, dry, red, or brownish-gray skin that may weep fluid and eventually crust over during flare-ups.
The rash most commonly develops in the flexural areas of the body — the creases of the elbows, the back of the knees, the wrists, ankles, and around the neck. In infants, eczema often first appears on the cheeks and forehead. In older children and adults, it tends to concentrate in the elbow and knee creases.
What makes eczema recognizable in pictures is the combination of redness, lichenification (skin thickening from chronic scratching), and a notable dryness that can cause visible flaking. During active flares, small fluid-filled vesicles (tiny blisters) may appear within the rash, particularly on the hands and feet in a variant called dyshidrotic eczema.
Color-wise, eczema appears bright red to dark red in fair skin tones, and hyperpigmented (darker than surrounding skin) or even hypopigmented in darker complexions — a critical distinction that photographs must account for across diverse skin tones.
Eczema is a chronic, relapsing condition. Between flares, the skin may appear normal, but triggers such as sweat, heat, soaps, fabrics, pet dander, and stress can rapidly reinitiate the inflammatory cascade.
Symptom Checklist
- Intense itching, often worse at night
- Dry, sensitive skin that may crack
- Red to brownish-gray patches
- Small, raised bumps that may weep fluid
- Thickened, scaly, or cracked skin
- Raw, swollen skin from scratching
- Common in elbow and knee creases
- Possible facial involvement in infants
- Rash covers a large portion of your body
- Signs of skin infection: oozing, crusting, fever
- Severe sleep disruption due to itching
- Rash does not improve with OTC treatments within 2 weeks
- New rash in an infant under 3 months
Psoriasis Rash Pictures
Psoriasis is a chronic autoimmune condition that fundamentally alters the skin cell cycle, causing cells to build up rapidly on the skin's surface — forming scales and red patches that can be itchy and sometimes painful. In photographs, psoriasis presents as some of the most visually distinctive skin lesions in dermatology, making it relatively identifiable with the right visual education.
The hallmark of plaque psoriasis — the most common form, accounting for about 80–90% of cases — is well-defined, raised red or salmon-colored plaques covered by silvery-white scales. These plaques typically appear symmetrically on the body, preferring extensor surfaces: the elbows, knees, lower back, and scalp. The scalp is involved in approximately 50% of cases and can be a challenging area to treat.
In photographs, the silvery scale is the key identifier. This scale develops because the immune system mistakenly signals skin cells to regenerate every 3–4 days instead of the usual 28–30 days — resulting in a rapid accumulation of cells on the surface. When the scale is gently removed, a characteristic pinpoint bleeding phenomenon called the Auspitz sign may be observed.
Guttate psoriasis presents quite differently — as small, drop-shaped lesions that are less scaly and often follow a streptococcal throat infection, particularly in younger patients. Inverse psoriasis appears as smooth, shiny red patches in body folds rather than with scales. These subtypes each have distinct visual signatures worth knowing.
Psoriasis can also involve the nails (nail pitting, oil spots, onycholysis) and the joints (psoriatic arthritis), and monitoring for these associated findings is clinically important beyond just skin assessment.
Symptom Checklist
- Raised, inflamed red or salmon-colored plaques
- Thick silvery-white scale covering plaques
- Symmetrical distribution on body
- Commonly on elbows, knees, scalp, lower back
- Nail changes: pitting, discoloration
- Itching and burning sensation
- Joint pain or stiffness (psoriatic arthritis)
- Skin cracking and bleeding at edges
- More than 10% of body surface area is affected
- Sudden widespread guttate psoriasis eruption
- Joint swelling or pain alongside skin symptoms
- Pustular or erythrodermic psoriasis (red all over)
- Current treatment has stopped working
Viral Rash Pictures
Viral rashes, or exanthems, are skin eruptions that occur as a direct or immune-mediated response to a viral infection. They are among the most common reasons children and adults seek medical attention for skin changes, and their correct identification is clinically significant because different viral rashes carry different implications for contagiousness, severity, and management.
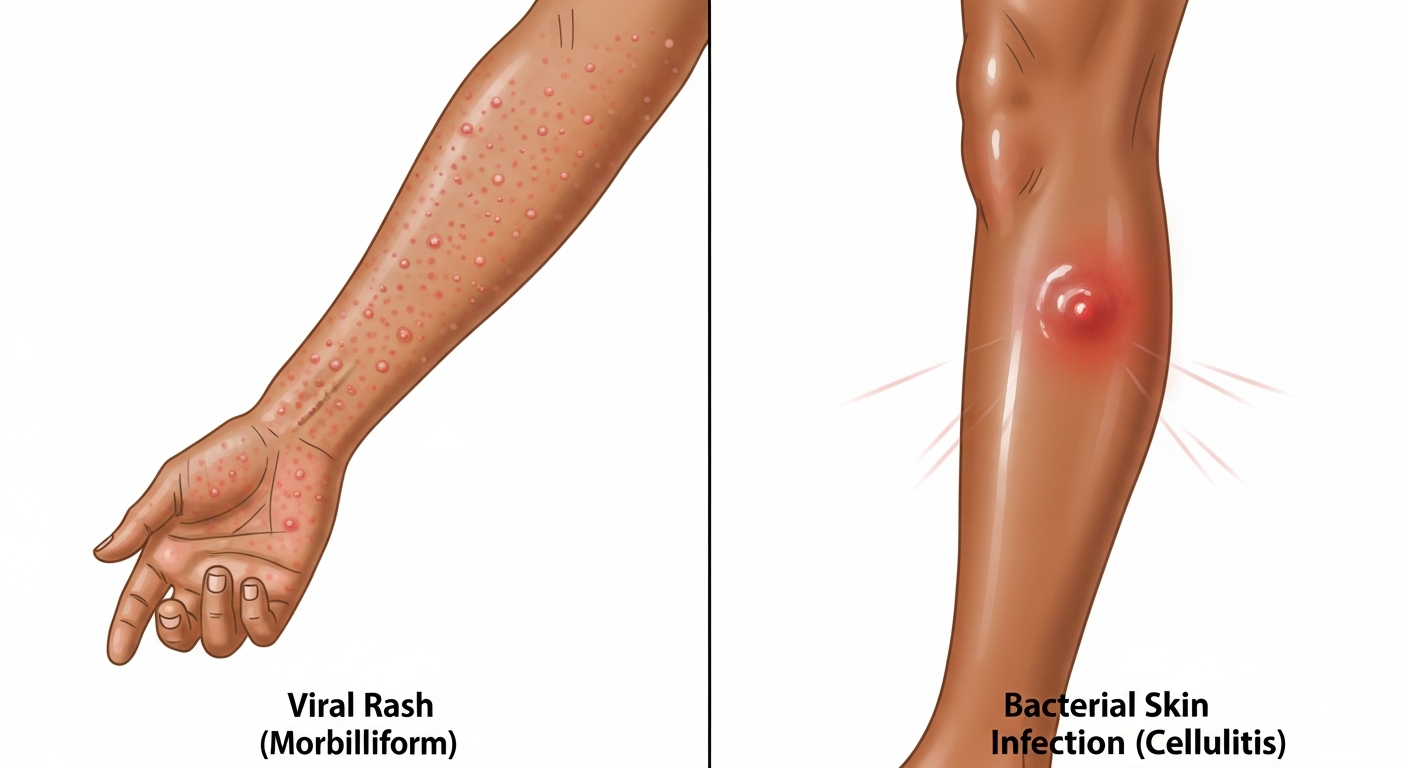
Visually, viral rashes span a wide spectrum. Measles (rubeola) produces a characteristic maculopapular rash — flat red spots that merge — starting on the face near the hairline and spreading down the body over 2–4 days. Rubella produces a similar but milder, shorter-lived rash. Roseola infantum causes a high fever followed by a sudden appearance of a pink, blotchy rash on the trunk as the fever breaks — a pattern so distinctive it is nearly pathognomonic.
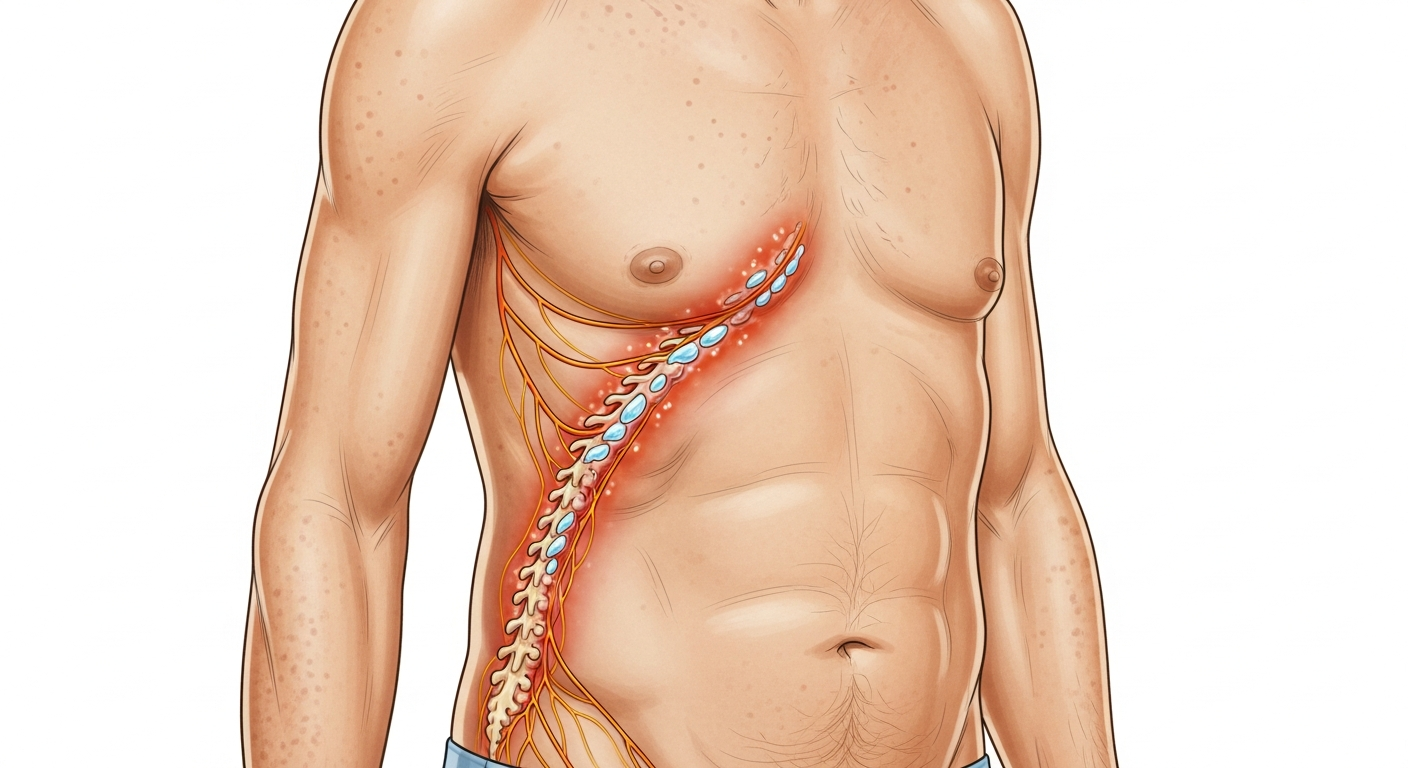
Chickenpox (varicella) is particularly identifiable: it progresses through stages from red macules to papules to fluid-filled vesicles to crusted lesions — crucially, all stages are present simultaneously, which is a key photographic identifier. Shingles (herpes zoster), caused by reactivation of the same varicella virus, appears as a painful, unilateral band of vesicles following a dermatome.
Enteroviral rashes (such as from Coxsackievirus in hand, foot, and mouth disease) produce vesicles specifically on the palms, soles, and inside the mouth. The location is the key identifier in photographs.
Fifth disease (parvovirus B19) produces the classic "slapped cheek" appearance in children — bright red cheeks — followed by a lacy, reticular rash on the extremities. Recognizing this pattern avoids unnecessary alarm and guides appropriate infection control measures, particularly in pregnant individuals.
Symptom Checklist
- Widespread red or pink spots (macules/papules)
- Rash often starts on face or trunk and spreads
- Accompanied by fever, fatigue, or sore throat
- Multiple rash stages may be present simultaneously
- Can affect mucous membranes
- May be mildly or severely itchy
- Duration typically 3–7 days
- May have prodromal symptoms before rash appears
- Rash with high fever above 39°C (102°F) in children
- Non-blanching (petechial/purpuric) rash — possible meningitis
- Rash in a pregnant individual (risk of parvovirus B19)
- Severe chickenpox in adults or immunocompromised
- Widespread blistering or mucous membrane involvement
Fungal Rash Pictures

Fungal skin infections — collectively referred to as tinea infections or dermatomycoses — are caused by dermatophytes (fungi that infect keratin-rich tissues), yeasts such as Candida, or molds. They are extremely common, highly contagious through direct contact, and visually distinctive enough that photographic guides significantly improve early identification and management.
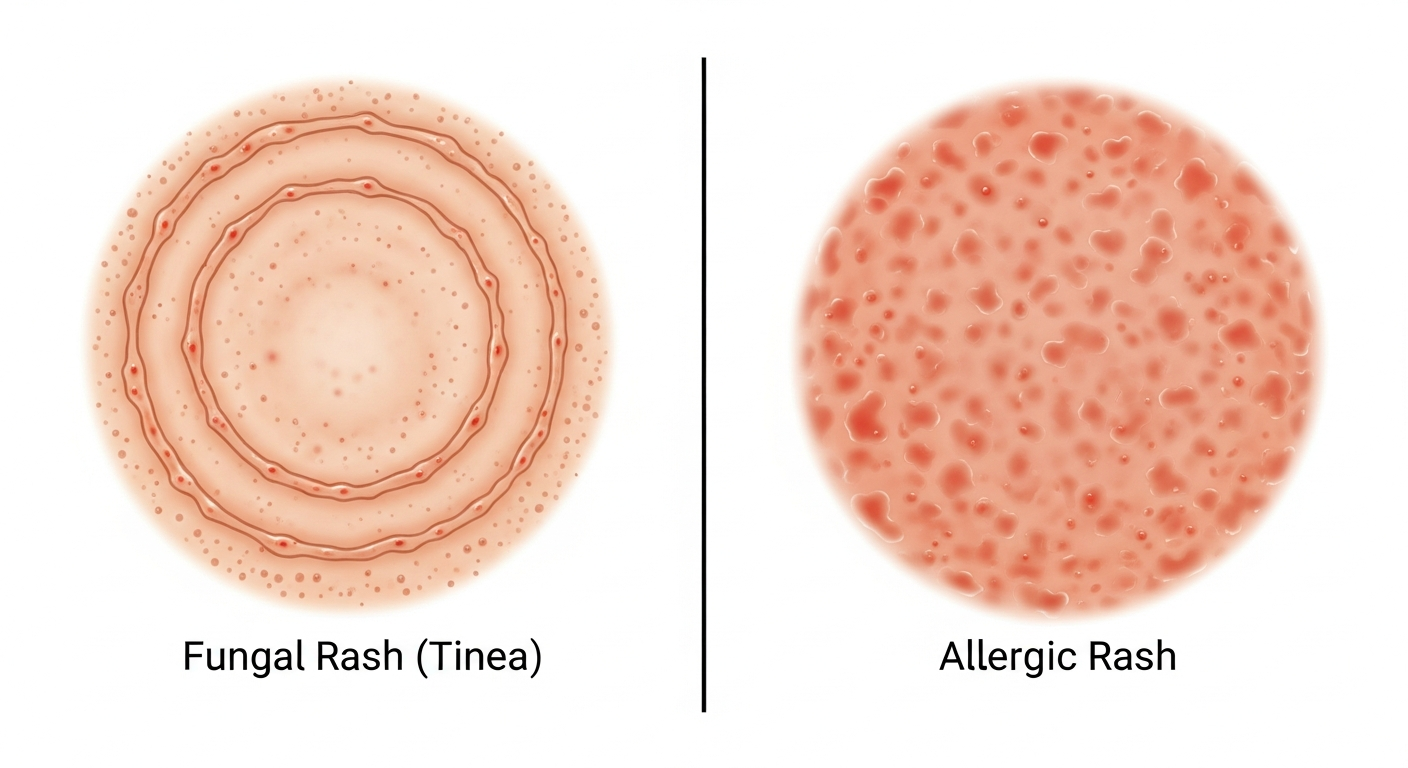
Tinea corporis (ringworm of the body) is the prototypical fungal rash in photographs: a circular or annular (ring-shaped) lesion with a scaly, raised, active border and a relatively clear or hyperpigmented center. The ring shape is caused by the centrifugal spread of the fungus from the initial infection point, with the outer edge representing the active growth front. Multiple rings may coalesce into complex patterns.
Tinea pedis (athlete's foot) appears in photographs as maceration (white, soggy skin) between the toes, scaling along the sides of the feet, or in a "moccasin distribution" covering the soles. Tinea cruris (jock itch) appears as a red, scaly rash in the groin area with a distinct advancing border. Tinea capitis affects the scalp and is a leading cause of non-scarring alopecia in children.
Candidal intertrigo presents differently — as bright red, moist rash in body folds (armpits, beneath breasts, groin, between fingers) often with surrounding "satellite pustules" — small pustules at the edge of the main rash that are characteristic of Candida specifically.
Tinea versicolor, caused by Malassezia yeasts, produces hypo- or hyperpigmented macules — lighter or darker patches — on the trunk and upper arms, particularly noticeable after sun exposure. This discoloration can persist months after successful treatment.
Symptom Checklist
- Ring-shaped, circular lesions (tinea corporis)
- Scaly, raised active border with clearer center
- Intense itching at site of infection
- Skin maceration and scaling between toes (athlete's foot)
- Red moist rash in skin folds with satellite pustules (Candida)
- Discolored patches (lighter or darker) on trunk
- Fragile, brittle hair or patchy hair loss on scalp
- Spreads with scratching or skin-to-skin contact
- Scalp involvement or hair loss in a child
- Rash spreading rapidly despite OTC antifungal treatment
- Diabetic or immunocompromised with widespread fungal rash
- Nails are yellow, thickened, or separating from nail bed
- Infection affecting the face or eyes
Allergic Rash Pictures

Allergic skin reactions produce some of the most varied and rapidly changing rashes in dermatology, ranging from localized contact reactions to generalized hives and, in severe cases, angioedema. Understanding what allergic rashes look like in photographs is essential for distinguishing them from infectious or autoimmune causes — and for recognizing when an allergic reaction becomes a medical emergency.
Allergic contact dermatitis occurs when the skin is directly exposed to a sensitizing substance. Classic triggers include nickel (from jewelry), poison ivy (urushiol), latex, fragrances, preservatives, and topical antibiotics. In photographs, allergic contact dermatitis appears as a geometric or shape-specific rash that precisely mirrors the area of contact — a linear streaking pattern from poison ivy, a watchband-shaped rash from nickel, a waistband-shaped rash from rubber elastic.
The reaction may appear 24–72 hours after exposure (delayed hypersensitivity), typically as redness, swelling, and vesicle formation that can be intensely itchy. This time delay is a key diagnostic point and helps distinguish it from irritant contact dermatitis, which develops immediately.
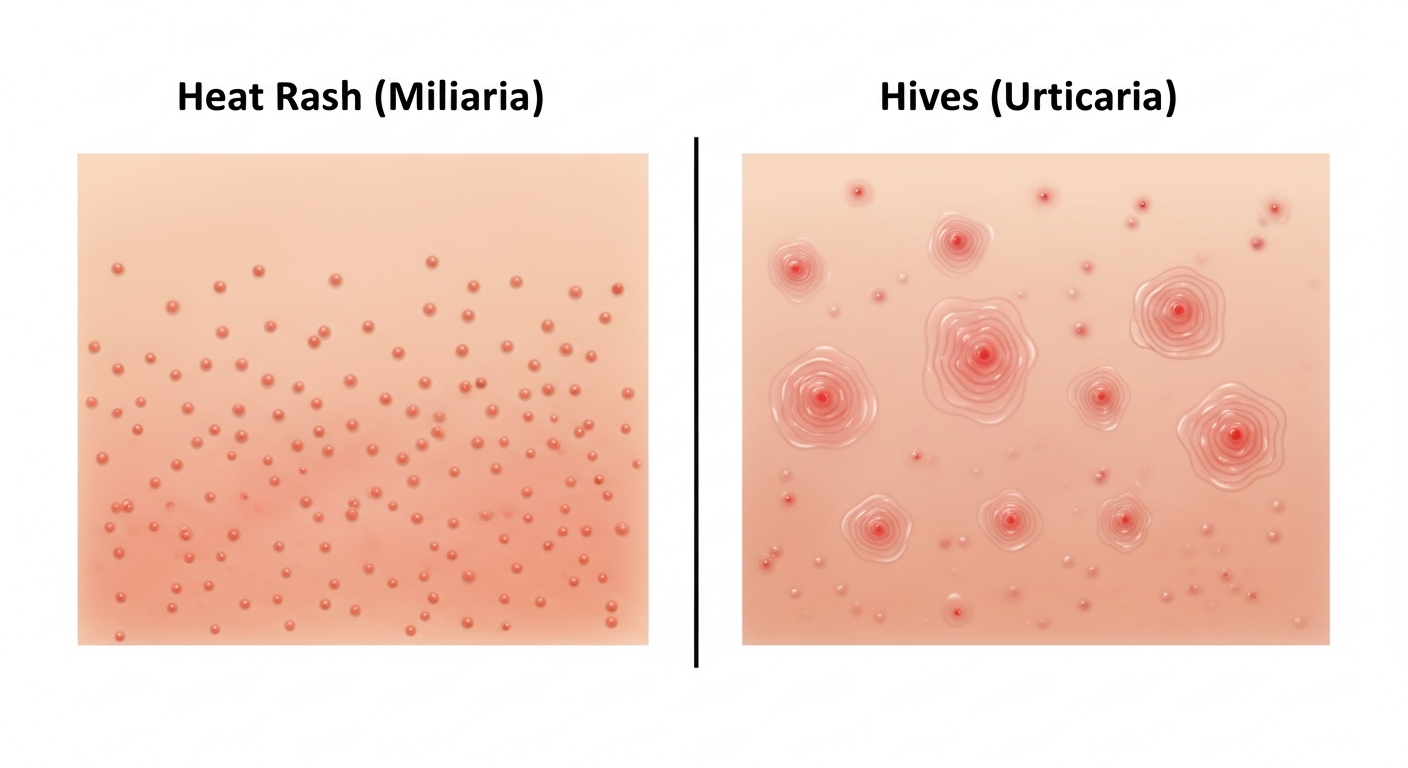
Urticaria (hives) is the most classic allergic rash in terms of visual presentation. In photographs, hives appear as raised, erythematous wheals — elevated welts with a pale center and red flare — that characteristically move and change location within hours. This migratory behavior is highly distinctive and represents the hallmark of true urticaria.
Atopic dermatitis (eczema) exists on the allergic spectrum and involves IgE-mediated sensitization. Drug rashes from antibiotics (commonly amoxicillin) or other medications produce widespread morbilliform (measles-like) rashes or, rarely, severe reactions including Stevens-Johnson syndrome with mucosal involvement.
Symptom Checklist
- Raised, itchy welts (hives) that shift location
- Redness precisely matching allergen contact area
- Vesicles, blisters, or oozing at contact site
- Swelling of lips, eyes, or throat (angioedema)
- Widespread morbilliform rash after medication
- Intense itch appearing 24–72 hours after exposure
- Hives appearing within minutes of allergen exposure
- Skin may feel hot and look sunburned
- Throat swelling, hoarseness, or difficulty swallowing
- Difficulty breathing or wheezing alongside rash
- Rash following recent vaccination or new medication
- Lip or tongue swelling (angioedema)
- Hives persisting for more than 6 weeks
Heat Rash Pictures
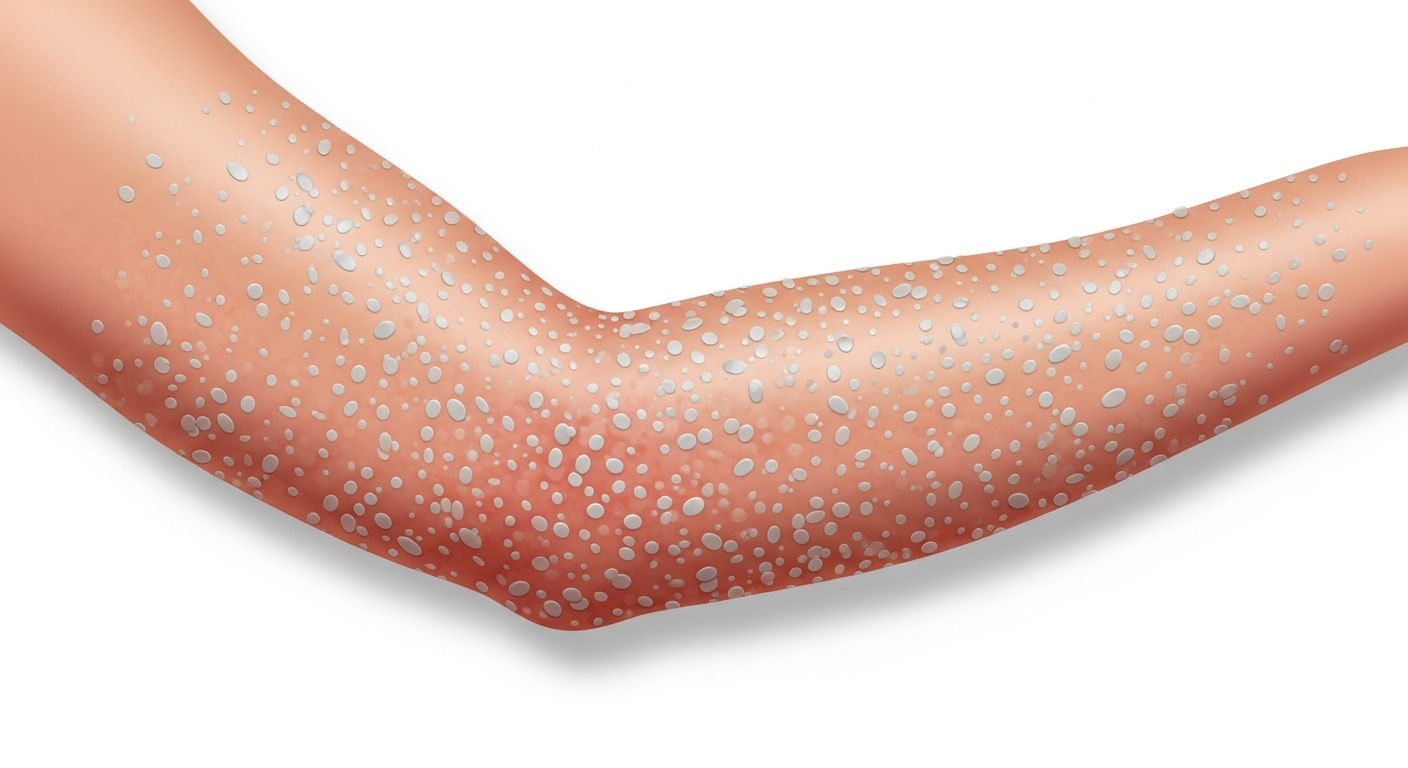
Heat rash, medically termed miliaria, develops when sweat ducts become blocked, trapping perspiration beneath the skin and triggering an inflammatory response. It is one of the most common summer rashes and is particularly prevalent in infants whose immature sweat glands are easily occluded. In photographs, heat rash presents along a spectrum depending on the depth of sweat duct blockage.
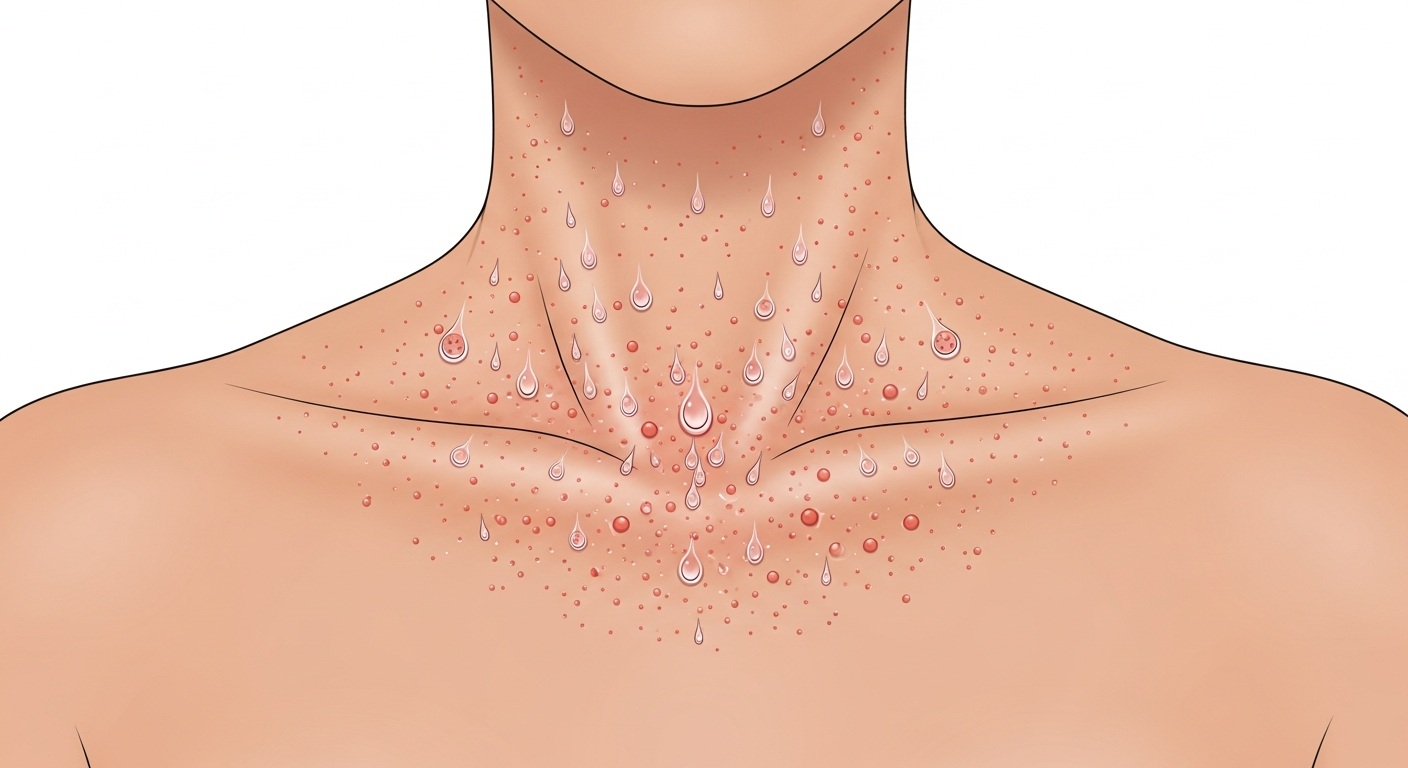
Miliaria crystallina — the mildest form — appears as tiny, clear or white, superficial blisters resembling water droplets on the skin surface. They are fragile and rupture with light friction. In photographs, these look like a field of translucent seed-like bumps, typically on the trunk.
Miliaria rubra (prickly heat) — the most common and symptomatic form — appears as small red papules or vesicles surrounded by red halos in areas of friction and heat: the neck, upper chest, elbow creases, and groin. The red color and prickly, itchy sensation give this form its common name. In photographs, it resembles a fine red bumpy rash concentrated in warm, covered skin folds.
Miliaria pustulosa occurs when miliaria rubra becomes secondarily infected, developing pustular tops. Miliaria profunda, the deepest and least itchy form, produces flesh-colored papules that are harder to identify visually without clinical context.
Heat rash is almost always provoked by a clear trigger — hot and humid weather, fever, overdressing (particularly in infants), or intense exercise — and typically resolves within hours to days of cooling the skin, which is a key distinguishing feature from chronic inflammatory rashes.
Symptom Checklist
- Tiny red bumps or blisters on skin surface
- Appears in skin folds, neck, chest, groin, armpits
- Prickly or stinging sensation (prickly heat)
- Worsens with heat and sweating
- Common in infants, physically active adults
- Resolves within hours to days of cooling
- May become pustular if secondarily infected
- Non-contagious — caused by blocked sweat ducts
- Rash becomes pustular (signs of skin infection)
- Fever accompanying the rash in an infant
- Heat rash doesn't resolve within 3–4 days
- Signs of heat exhaustion: dizziness, nausea
- Rash spreading rapidly beyond expected areas
Bacterial Rash Pictures
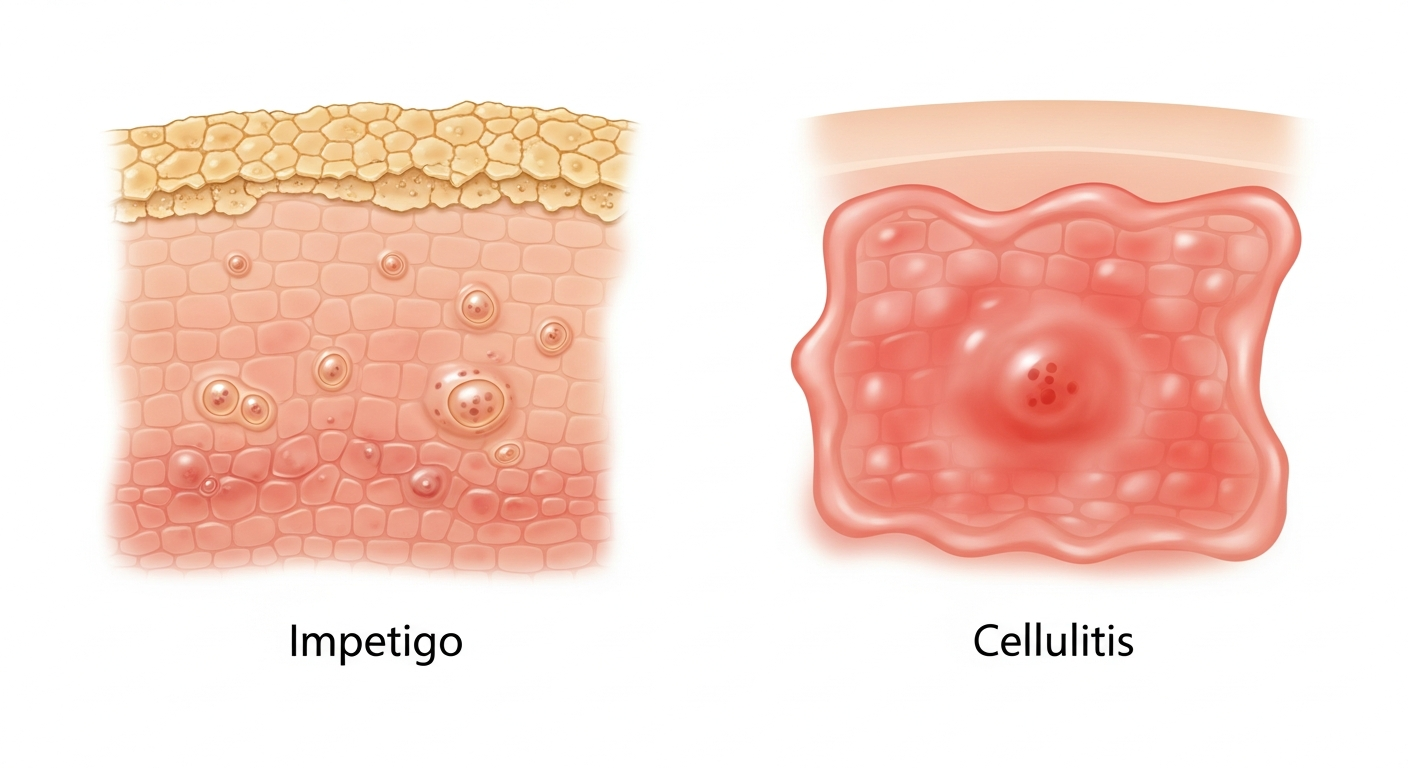
Bacterial skin infections produce a diverse range of rashes, from the superficial honey-crusted lesions of impetigo to the deep, spreading redness of cellulitis and the widespread sandpaper rash of scarlet fever. Recognizing bacterial rashes is critically important because most require antibiotic treatment and some — such as septicemia — are life-threatening.
Impetigo is the most common bacterial skin infection in children and one of the most visually distinctive. In photographs, non-bullous impetigo (caused by Staphylococcus aureus or Streptococcus pyogenes) shows clusters of small blisters that rupture quickly, leaving behind characteristic honey-colored, golden crusts on the skin. These crusts are a near-pathognomonic finding — yellowish, sticky crusting on a red base. Bullous impetigo (caused by S. aureus) shows larger, fluid-filled blisters that don't rupture as quickly.
Cellulitis is a deep skin infection that appears in photographs as a large, poorly-demarcated area of redness, warmth, and swelling — typically on the lower legs. Unlike a rash, cellulitis doesn't have distinct borders and spreads progressively. The skin may appear shiny and taut. Red streaking (lymphangitis) extending from the rash toward the body is a sign of spreading infection requiring urgent care.
Scarlet fever, caused by Group A Streptococcus, produces the characteristic "sandpaper rash" — fine, red, gooseflesh-like bumps that produce a rough texture to touch. In photographs, it appears as widespread erythema with a pebbled texture, beginning on the trunk and spreading outward, with the face typically showing "strawberry tongue" and flushed cheeks sparing the area around the mouth (circumoral pallor).
Erysipelas is a superficial bacterial infection showing a bright, fiery red, sharply demarcated plaque — typically on the face or lower legs — that is raised and has a clear border distinguishing it from normal skin.
Symptom Checklist
- Honey-colored golden crusts (impetigo)
- Large spreading area of red, warm, swollen skin
- Sandpaper texture rash (scarlet fever)
- Red streaking extending from rash (lymphangitis)
- Blistering with surrounding redness
- Fever accompanying skin changes
- Painful, tender skin over infected area
- Possible pus, abscess, or weeping

- Any suspected cellulitis — requires antibiotics
- Red streaking from wound site toward body
- Rapid expansion of redness on the skin
- High fever with skin rash
- Impetigo in school-age child (highly contagious)
Parasitic Rash Pictures
Parasitic skin infestations are caused by mites, lice, fleas, bedbugs, and other external parasites that burrow into or feed on the skin, triggering intense immune reactions. Visually identifying these rashes is important because they spread between household members and require coordinated treatment of both affected individuals and their environment.
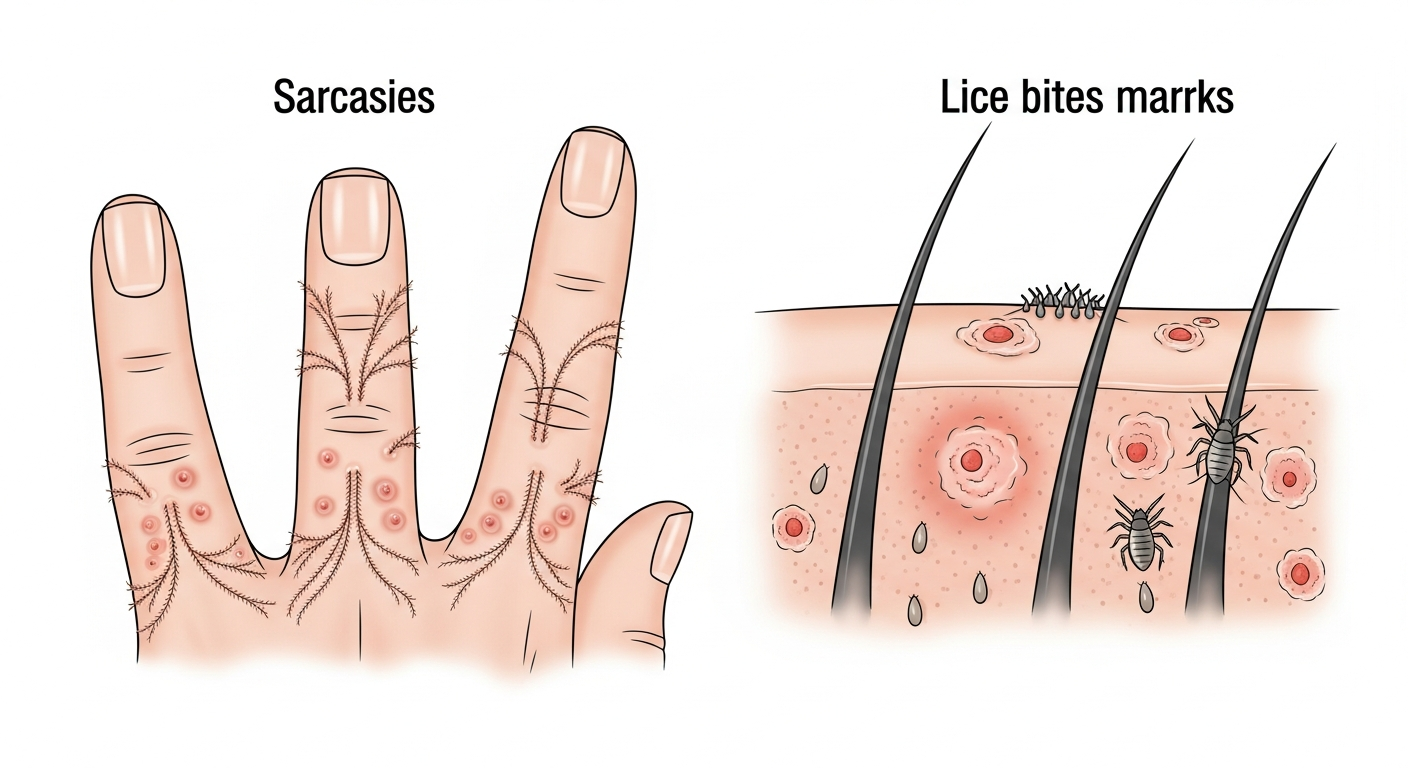
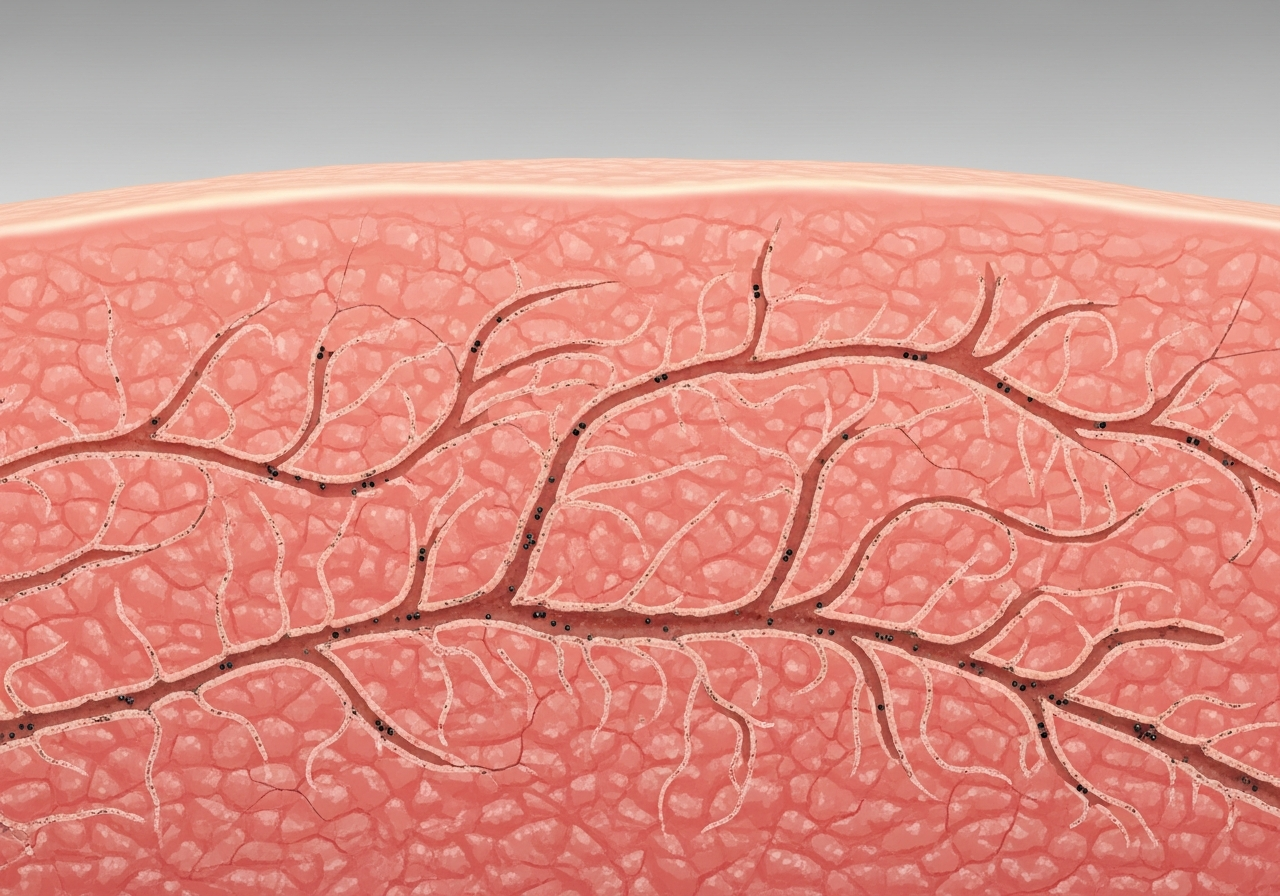
Scabies, caused by the mite Sarcoptes scabiei, is one of the most diagnostically distinctive parasitic rashes in photographs. The pathognomonic finding is the burrow — a thin, grayish or skin-colored wavy line of 5–15mm appearing in the webbing between fingers, on wrists, elbows, genitalia, and the beltline. These burrows represent the tunnels dug by the female mite to lay eggs. Surrounding the burrows is an intensely itchy, excoriated papular rash — the body's immune response to mite proteins. The itch of scabies characteristically worsens dramatically at night.
Lice produce bites that appear as small red papules, often with evidence of nits (eggs) attached to hair shafts — most commonly on the scalp, pubic area, or along seams of clothing (body lice). Lice bites on the scalp lead to excoriation and potential secondary bacterial infection visible as oozing and crusting in photographs.
Bedbug bites typically appear in linear or clustered groups of 3 bites (often described as "breakfast, lunch, and dinner") on exposed skin areas — arms, neck, and face. The bites are red, flat to slightly raised papules that become intensely pruritic. The pattern and location help distinguish them from random insect bites.
Flea bites produce small, clustered red papules typically on the lower legs and ankles, often with a central punctum visible on close examination. A linear or grouped pattern combined with pet exposure is highly suggestive.
Symptom Checklist
- Thin wavy burrow lines between fingers (scabies)
- Intense itching worsening at night (scabies hallmark)
- Small red papules in lines or clusters
- Nits (eggs) attached to hair shafts (lice)
- Bites in groups of 3 on exposed skin (bedbugs)
- Clustered bites on lower legs and ankles (fleas)
- Household members reporting similar symptoms
- Excoriation marks from intense scratching
- Suspected scabies — requires prescription treatment
- Multiple household members symptomatic
- Crusted (Norwegian) scabies in elderly or immunocompromised
- Secondary bacterial infection from scratching
- Lice in school-aged children with household contacts
Master Rash Comparison Table
A quick-reference clinical chart comparing all eight rash types covered in this visual guide across key diagnostic dimensions.
| Rash Type | Color | Texture | Itch Level | Contagious? | Typical Duration |
|---|---|---|---|---|---|
| Eczema | Red/brown | Dry, scaly, lichenified | Severe | No | Chronic/recurring |
| Psoriasis | Red with silver | Thick, scaly plaques | Moderate | No | Chronic/recurring |
| Viral Rash | Pink to red | Flat macules/papules | Mild–Moderate | Yes (virus) | 3–10 days |
| Fungal | Red, may scale | Scaly border, clear center | Moderate | Yes (contact) | Weeks if untreated |
| Allergic | Red/pink | Raised welts, smooth | Severe | No | Hours to days |
| Heat Rash | Red | Fine, prickly bumps | Mild–Moderate | No | Hours to 3 days |
| Bacterial | Red, may crust | Warm, tender, crusted | Mild (painful) | Yes (contact) | Days–weeks |
| Parasitic | Red | Papules, linear burrows | Severe at night | Yes (contact) | Weeks if untreated |
Frequently Asked Questions
Expert answers to the most common questions about visual rash identification and the reliability of rash pictures.
Explore Detailed Rash Guides
Medical Disclaimer: The visual examples, descriptions, and educational content on this page are for informational purposes only and do not constitute medical advice, diagnosis, or treatment. Skin conditions can look similar across different diseases and vary significantly by skin tone and stage of disease. Always consult a qualified dermatologist or healthcare professional for proper diagnosis and treatment of any skin condition. Read our full medical disclaimer.