Skin Rash Symptoms Guide: How to Recognize Mild vs Serious Rashes
Skin rashes are among the most common reasons people seek medical attention, affecting over one-third of the population at any given time. A rash is not a diagnosis — it is a symptom: the visible expression of an underlying process that can range from benign skin irritation to a serious systemic illness. Understanding what your rash symptoms mean is the first and most important step toward getting the right care.
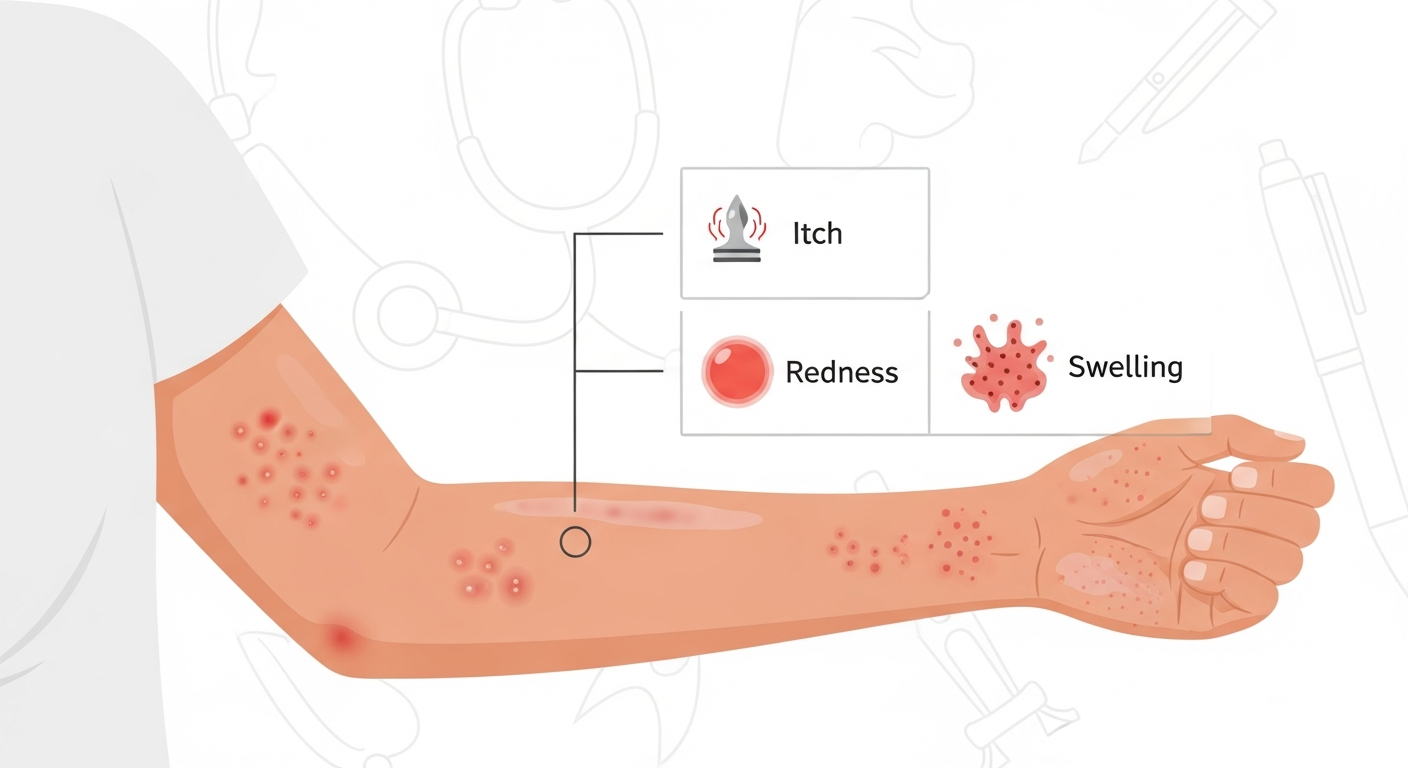
Rash symptoms develop through several distinct pathological pathways. Immune-mediated rashes occur when the immune system releases histamine, cytokines, and other inflammatory mediators in response to allergens, infections, or self-antigens — producing the redness, swelling, and itch that characterize most common rashes. Infectious rashes arise from direct skin invasion by bacteria, viruses, fungi, or parasites triggering local and systemic immune responses. Chronic inflammatory conditions such as eczema and psoriasis involve dysregulated immune activation that creates persistent skin inflammation without a conventional infectious trigger.
This guide covers the eight most clinically significant rash symptoms in depth — itching, burning, pain, blistering, scaling, spreading, fever, and swelling — along with a diagnostic framework based on body location, emergency warning signs, and prevention strategies. Each section provides evidence-based next steps appropriate to the severity of each symptom constellation.
While this guide is designed to be your most comprehensive educational resource for rash symptoms, it does not replace clinical evaluation. Many rash symptoms overlap between conditions, and a dermatologist has access to diagnostic tools — dermoscopy, skin biopsy, patch testing, and laboratory analysis — that extend far beyond what any symptom guide can offer. Use this page to become an informed patient, recognize warning signs, and have better conversations with your healthcare provider.
Itching Rashes
Mild RiskItching — medically termed pruritus — is the most common symptom associated with skin rashes and serves as a key diagnostic signal. It arises when mast cells and other immune cells release histamine and cytokines in the skin, stimulating itch-specific nerve fibers (C-fibers) that transmit signals to the brain. The intensity, pattern, and timing of itch provide important diagnostic clues.
Mild generalized itching that comes and goes, is easy to ignore during the day, and does not disturb sleep is generally low concern. However, severe, unrelenting itching — especially at night (nocturnal pruritus) — raises concern for conditions such as scabies, cholestasis (bile salt accumulation), or lymphoma. Itch without any visible rash at all is a recognized symptom of systemic disease and warrants medical evaluation.
Contact with known irritants, new fabrics, detergents, or personal care products is the most common trigger for isolated itching rashes. Eczema, hives (urticaria), and allergic contact dermatitis all produce intense pruritus. Psoriasis typically causes milder, intermittent itch compared to eczema. Identifying the pattern — whether itch precedes the rash or follows it — helps distinguish primary dermatological from systemic causes.
Possible Causes
- Eczema (atopic dermatitis)
- Hives (urticaria)
- Contact dermatitis
- Scabies mite infestation
- Psoriasis
- Dry skin (xerosis)
- Liver or kidney disease (systemic pruritus)
- Drug reactions
Recommended Next Steps
- Apply fragrance-free moisturizer and cool compresses
- Try OTC antihistamine (cetirizine or loratadine)
- Avoid scratching — use a cold pack instead
- See a doctor if itching persists beyond 2 weeks or is nocturnal
- Keep a symptom diary tracking triggers
Burning Rashes
Moderate RiskA burning sensation accompanying a rash suggests a different pathological mechanism than itch — typically nerve involvement, superficial tissue damage, or a more intense inflammatory response. Unlike itch, which signals the urge to scratch, burning pain often signals direct nerve stimulation or skin barrier compromise.
The most clinically important cause of a burning rash is shingles (herpes zoster). This condition presents with a unilateral, burning, painful rash confined to a single dermatome — following the path of a nerve — that begins as redness and progresses to clusters of vesicles. The burning pain in shingles can precede visible skin changes by 2–4 days, leading to diagnostic delay. Recognition and early antiviral treatment within 72 hours of vesicle onset significantly reduces the risk of post-herpetic neuralgia (long-term burning nerve pain).
Other causes of burning rashes include contact with irritant chemicals or plants (chemical burns, poison ivy), sunburn (UV radiation damaging skin cells), first-degree burns, and certain drug reactions. Rosacea produces a burning sensation in the facial skin alongside redness and flushing. Burning mouth syndrome and vulvodynia are localized burning pain conditions without visible rash that require specialist evaluation.
Possible Causes
- Shingles (herpes zoster)
- Sunburn
- Chemical or plant contact burns
- Rosacea
- Drug hypersensitivity reactions
- Cutaneous lupus
- Radiation dermatitis
- Peripheral neuropathy with skin changes
Recommended Next Steps
- Seek medical attention promptly for unilateral burning with blistering
- Cool (not cold) water for burns — do not apply ice
- Antiviral treatment for shingles is most effective if started within 72 hours
- Avoid further sun exposure and apply broad-spectrum SPF 50+
- Keep burned skin clean and moist with gentle dressings
Painful Rashes
Moderate RiskPain is not the most common rash symptom, but when a rash is painful — tender to touch, throbbing, or producing stabbing sensations — it usually indicates a more serious underlying process than a simple inflammatory skin condition. Pain in a rash most often signals infection, nerve involvement, or deep tissue inflammation.
Cellulitis is the archetypal painful rash: a spreading bacterial skin infection that produces a warm, red, swollen, and distinctly tender area — most commonly on the lower legs. It is caused by Streptococcus or Staphylococcus bacteria entering through a skin break. The tenderness, warmth, and spreading borders over hours to days are clinical hallmarks. Without treatment with antibiotics, cellulitis can spread to the lymph nodes and bloodstream.
Erysipelas is a related but more superficial bacterial infection producing a sharply demarcated, fiery red, raised, and painful plaque — typically on the face or lower legs. Abscesses produce throbbing, focal pain with a fluctuant (soft, pus-filled) center. Necrotizing fasciitis, a rare but life-threatening deep infection, produces pain disproportionate to the visible skin findings — severe internal pain with relatively mild surface changes — and constitutes a surgical emergency.
Vasculitic rashes (from immune complex deposition in blood vessel walls) can be painful, particularly palpable purpura on the lower legs. Painful mouth ulcers alongside a rash may indicate Behçet's disease or Stevens-Johnson syndrome.
Possible Causes
- Cellulitis (bacterial skin infection)
- Shingles (pre-vesicular pain)
- Erysipelas
- Abscess or furuncle
- Vasculitis (inflamed blood vessels)
- Stevens-Johnson syndrome
- Necrotizing fasciitis (emergency)
- Contact burns or chemical exposure
Recommended Next Steps
- Seek same-day care for any warm, spreading, tender rash
- Mark the border of redness with a pen — expanding border is an emergency
- Do not attempt to drain a painful abscess at home
- Antibiotics are required for bacterial causes — do not delay
- Any rash with disproportionate pain requires emergency evaluation
Blistering Rashes
Severe RiskBlisters (vesicles when small, bullae when large) form when fluid accumulates between skin layers due to friction, burns, immune attack on skin proteins, or viral infection. The cause of blistering determines both treatment and urgency — blisters from friction are benign, while blisters from autoimmune disease or drug reactions can be life-threatening.
Chickenpox (varicella) produces one of the most recognizable blistering patterns: crops of vesicles on a red base ("dew drops on a rose petal" appearance) appearing in successive waves across the body, with all lesion stages present simultaneously. Shingles produces grouped vesicles in a dermatomal distribution. Herpes simplex (cold sores or genital herpes) produces clustered vesicles on an erythematous base at a consistent anatomical location.
Contact with poison ivy, poison oak, or poison sumac produces linear or geometric blistering at the contact site within 24–72 hours. Bullous impetigo causes large, fragile blisters filled with clear or turbid fluid. Pemphigus vulgaris is an autoimmune blistering disease where the immune system attacks the proteins holding skin cells together, causing painful erosions in the mouth and on the skin. Bullous pemphigoid, more common in the elderly, causes large, tense blisters that don't rupture as easily.
Stevens-Johnson syndrome and its severe form, toxic epidermal necrolysis (TEN), represent the most dangerous blistering reactions — typically triggered by medications — causing widespread skin detachment that requires intensive care.
Possible Causes
- Chickenpox (varicella)
- Shingles (herpes zoster)
- Herpes simplex virus
- Bullous impetigo
- Contact with plants (poison ivy)
- Pemphigus or bullous pemphigoid (autoimmune)
- Stevens-Johnson syndrome (drug reaction)
- Second-degree burns
Recommended Next Steps
- Do not pop or drain blisters — they protect the healing skin beneath
- Seek emergency care for blistering after starting a new medication
- Antiviral treatment for chickenpox or shingles is most effective early
- Consult a dermatologist for unexplained tense blisters
- Keep blistered areas clean and covered with non-adherent dressings
Scaling Rashes
Mild RiskScaling refers to the visible shedding of the outer layer of skin (stratum corneum) as dry, flaky particles. It develops when the normal process of skin cell turnover is accelerated, disrupted, or when the skin barrier is chronically compromised. While scaling is usually not a sign of serious illness, it is one of the most persistent and diagnostically informative rash symptoms.
Psoriasis produces the most characteristic and distinctive scaling of any common skin condition: thick, adherent, silvery-white scale overlying well-defined red plaques. The scale in psoriasis reflects an extremely accelerated cell cycle (3–4 days instead of the usual 28–30 days), producing more cells than the surface can shed normally.
Seborrheic dermatitis produces greasy, yellowish scale preferentially in sebaceous (oily) areas: the scalp, eyebrows, sides of the nose, and central chest. This distinguishes it from psoriasis, which favors dry, extensor surfaces. Dandruff is a mild form of seborrheic dermatitis affecting only the scalp.
Tinea versicolor (a yeast infection) produces fine scaling on discolored patches on the trunk and upper arms. Ichthyosis encompasses a group of genetic disorders producing widespread, fish-scale-like skin. Pityriasis rosea produces a distinctive "herald patch" followed by a widespread scaling eruption with a Christmas-tree distribution on the trunk. Eczema in its chronic, lichenified stage develops thickened, scaly skin from repetitive scratching.
Possible Causes
- Psoriasis (silvery scale)
- Seborrheic dermatitis (greasy scale)
- Eczema (chronic lichenification)
- Tinea versicolor (fine scale on discolored patches)
- Pityriasis rosea
- Ichthyosis (genetic scaling disorder)
- Dry skin (xerosis)
- Fungal infections (tinea corporis)
Recommended Next Steps
- Moisturize twice daily with a thick, fragrance-free cream or ointment
- OTC antifungal shampoos (ketoconazole) help seborrheic dermatitis on scalp
- See a doctor for rapidly spreading, thick, or pain-associated scaling
- Avoid very hot showers — use lukewarm water and gentle cleansers
- Prescription corticosteroids or biologics may be needed for psoriasis
Spreading Rashes
Moderate RiskA rash that is actively spreading — expanding its borders, appearing on new body parts, or increasing in density — requires prompt attention because spread can indicate an infectious process, a systemic allergic reaction, or the progression of an autoimmune condition. The rate and pattern of spread carry important diagnostic information.
Cellulitis is the most urgent cause of a spreading rash to recognize: if you mark the borders of a red, warm area on the skin and find it has expanded 2–4 hours later, this is a medical emergency requiring same-day antibiotic treatment. Impetigo spreads through autoinoculation — scratching and transferring bacteria to new sites.
Allergic reactions (urticaria) spread as new mast cells are triggered throughout the body, producing new hives in areas that weren't initially affected. Drug rashes characteristically start on the trunk and spread centrifugally outward over 24–48 hours. The morbilliform (measles-like) rash of drug hypersensitivity can cover the entire body within days.
Eczema flares can spread from the primary site to secondary areas through the process of sensitization. Contact dermatitis spreads if the allergen continues to contact new skin areas — such as cosmetics spreading to the neck during application.
A spreading rash with systemic symptoms (fever, fatigue, joint pain, mucous membrane involvement) should always be evaluated urgently, as it may represent a drug hypersensitivity syndrome (DRESS) or other serious systemic reaction.
Possible Causes
- Spreading cellulitis (bacterial — urgent)
- Urticaria (new hives appearing in multiple areas)
- Drug hypersensitivity rash
- Spreading impetigo (bacterial)
- Eczema flare with secondary sensitization
- Scabies (spreading infestion)
- DRESS syndrome (drug reaction)
- Systemic lupus rash
Recommended Next Steps
- Mark rash borders with a pen and check every 2 hours — expanding border is an emergency sign
- Stop any new medications recently started and consult a doctor
- Seek same-day care if spreading is rapid (hours) and skin is warm and tender
- Photograph the rash with timestamps to document spreading for your doctor
- Avoid spreading contact allergens to new areas — wash hands after touching rash
Rash with Fever
Severe RiskA rash accompanied by fever is one of the highest-priority symptom combinations in medicine. Fever indicates the immune system is mounting a systemic response — meaning the cause of the rash extends beyond the skin itself into the body's broader physiology. The combination narrows the differential diagnosis significantly and raises urgency.
In children, fever with rash is common and often represents viral infections: roseola (high fever then rash as fever breaks), chickenpox, measles, scarlet fever, hand-foot-and-mouth disease, and fifth disease all produce characteristic fever-rash pairings. While most of these are self-limiting, measles and scarlet fever require specific monitoring and treatment.
In adults, a new rash with high fever is more concerning and warrants urgent evaluation. Serious bacterial infections — particularly meningococcemia (meningococcal septicemia) — can present with fever and a rapidly progressive petechial or purpuric (non-blanching) rash. This combination is a medical emergency: a non-blanching rash with fever should be treated as meningococcemia until proven otherwise.
Rocky Mountain spotted fever (from tick bite) and other rickettsial diseases present with fever, headache, and a petechial rash beginning on the wrists and ankles and spreading centrally. Drug reaction with eosinophilia and systemic symptoms (DRESS) presents with rash, fever, lymph node swelling, and internal organ inflammation — a serious drug reaction requiring hospitalization.
Kawasaki disease, primarily affecting children under 5, presents with prolonged fever, rash, red eyes, cracked lips, and swollen lymph nodes — a vasculitis requiring urgent treatment to prevent coronary artery complications.
Possible Causes
- Viral exanthems (chickenpox, measles, roseola)
- Scarlet fever (Group A Streptococcus)
- Meningococcemia (emergency — non-blanching rash)
- Rocky Mountain spotted fever (tick-borne)
- DRESS drug reaction
- Kawasaki disease (children)
- Septicemia
- Adult-onset Still's disease
Recommended Next Steps
- Seek emergency care immediately for non-blanching (petechial) rash with fever
- Any fever above 39°C (102°F) with rash in a child requires same-day medical review
- Perform the glass test: press a glass against the rash — if spots don't fade, call emergency services
- Do not give aspirin to children with fever and rash (risk of Reye's syndrome)
- Document time of fever onset relative to rash appearance and tell your doctor
Rash with Swelling
Severe RiskSwelling accompanying a rash can range from localized puffiness (as in insect stings) to life-threatening angioedema affecting the airways. Understanding the location, speed of onset, and extent of swelling is critical to determining urgency. Swelling that involves the lips, tongue, throat, or eyes develops within minutes to hours and demands immediate evaluation.
Angioedema is deep swelling of the dermis and subcutaneous tissues, most commonly affecting the lips, eyelids, hands, feet, and genitalia. It can occur alone or alongside urticaria (hives). When angioedema involves the throat or tongue, it can obstruct the airway — a potentially fatal emergency requiring epinephrine and emergency care. Hereditary angioedema (HAE) is a rare genetic condition causing recurrent, non-allergic swelling episodes without hives.
Contact with insect stings, certain foods, medications (particularly ACE inhibitors and NSAIDs), or latex are common triggers of allergic angioedema. The swelling typically develops within 15–60 minutes of exposure and resolves within 24–72 hours with treatment.
Localized swelling over a warm, red, tender area (without hives) is more consistent with cellulitis — a bacterial infection requiring antibiotics. Lymphedema produces chronic, non-pitting swelling of an extremity from lymphatic system compromise and is typically non-inflammatory. Nephrotic syndrome (kidney disease) and heart failure produce bilateral pitting edema of the lower legs, which may be accompanied by skin changes including rashes from venous stasis.
Possible Causes
- Angioedema (allergic or hereditary)
- Insect sting or bite reaction
- Drug reaction (ACE inhibitors, NSAIDs, antibiotics)
- Cellulitis with perilesional edema
- Anaphylaxis (emergency)
- Lymphedema
- Contact dermatitis with prominent edema
- Venous stasis dermatitis
Recommended Next Steps
- Call emergency services immediately for throat, tongue, or lip swelling
- Use epinephrine auto-injector (EpiPen) if prescribed for known allergy
- Antihistamines alone are insufficient for severe angioedema — seek emergency care
- Document what you ate or touched in the 2 hours before swelling appeared
- Alert your doctor to any ACE inhibitor or NSAID use — consider switching medication
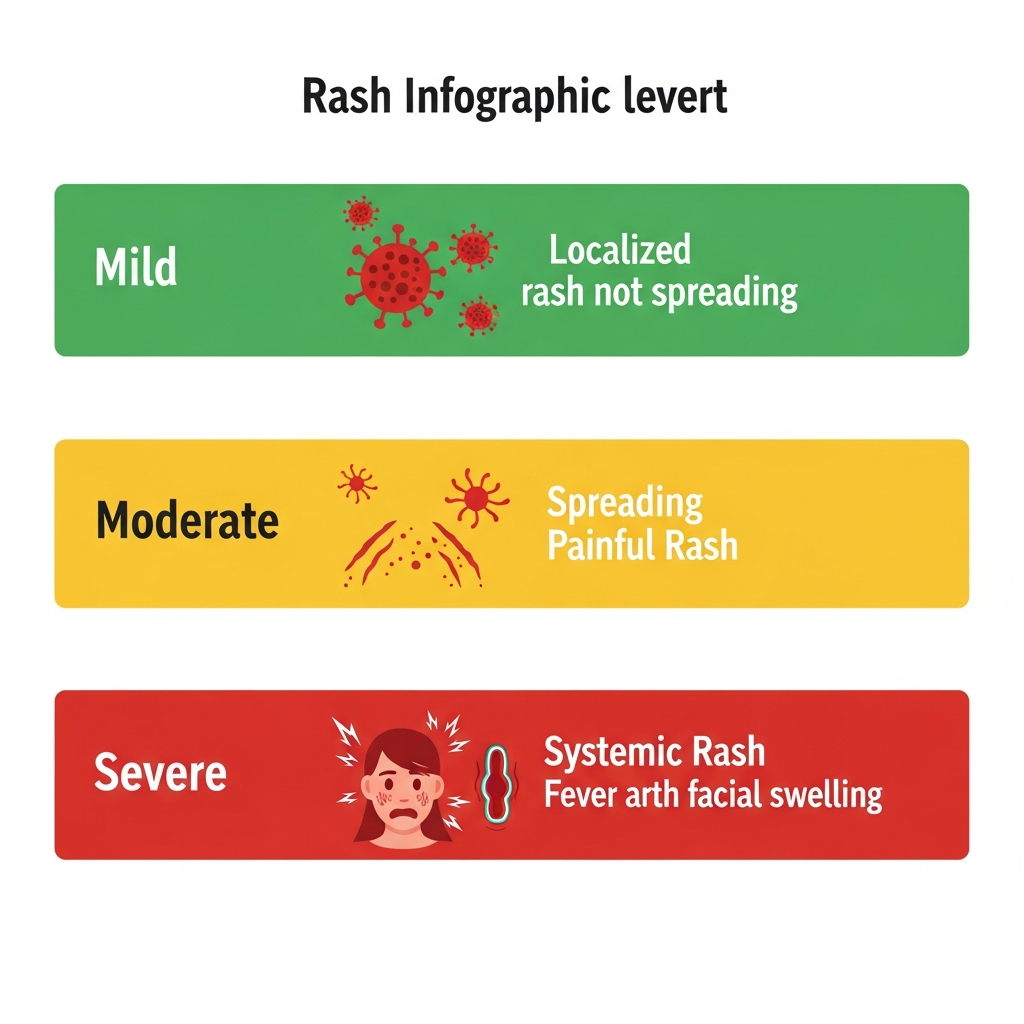
Symptom Severity Chart
Use this visual reference to quickly gauge the urgency of your rash symptoms. Combinations of symptoms raise severity — a mild rash that also has fever or rapid spreading moves into a higher risk category immediately.
| Symptom | Mild — Monitor at Home | Moderate — See a Doctor | Severe — Emergency |
|---|---|---|---|
| Itching | Minor, easy to ignore | Severe or nocturnal itch | Uncontrolled + rash spreading |
| Burning | Mild stinging, localized | Persistent burning rash | One-sided burn with blistering |
| Pain | Tender to touch only | Warm, spreading tenderness | Pain disproportionate to rash |
| Blistering | Small friction blisters | Blister rash after plant contact | Blistering after new medication |
| Scaling | Dry, flaky skin patches | Thick plaques not responding to OTC | Widespread skin peeling with pain |
| Spreading | Slow, small expansion | New areas affected over days | Rapid spread within hours |
| Fever | Low-grade fever (<38°C) | Moderate fever with rash | High fever + non-blanching spots |
| Swelling | Localized insect sting | Hives with local swelling | Throat, tongue, or lip swelling |
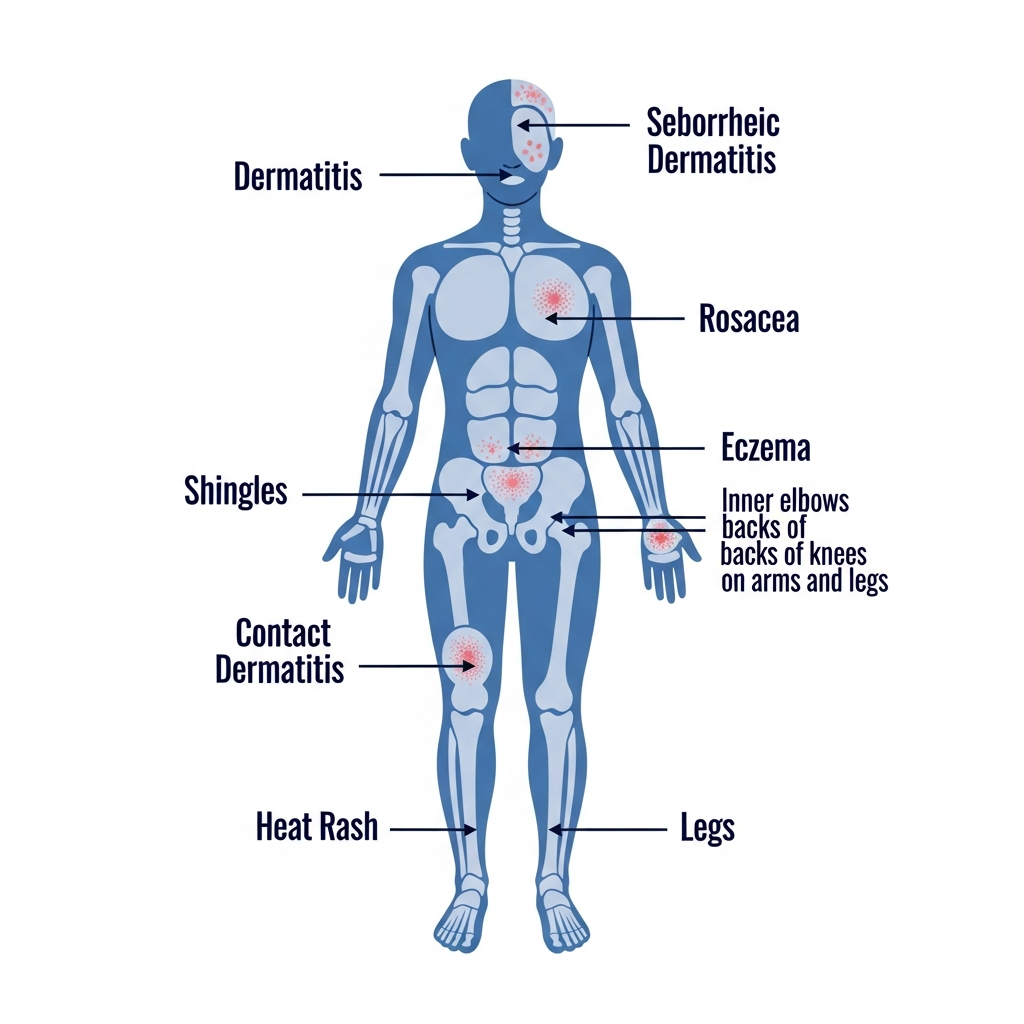
How Rash Location Helps Diagnosis
Where a rash appears on the body is one of the most important diagnostic clues available to dermatologists. Different skin conditions have strong predilections for specific anatomical locations based on factors including sebaceous gland density, friction, moisture, and UV exposure.
Face Rash
Common Causes
- Rosacea
- Seborrheic dermatitis
- Lupus (butterfly pattern)
- Acne
- Perioral dermatitis
- Contact allergy to cosmetics
Diagnostic Clue
Butterfly-shaped facial rash across the cheeks and nose is a hallmark of systemic lupus erythematosus and warrants immediate evaluation.
Facial Rash GuideArm Rash
Common Causes
- Eczema (inner elbow crease)
- Psoriasis (outer elbow)
- Contact dermatitis (from fabric or jewelry)
- Keratosis pilaris (upper arms)
- Sun-related rashes
Diagnostic Clue
Inner elbow crease rash strongly suggests eczema; outer elbow thick plaque favors psoriasis. Both are chronic but very manageable with correct treatment.
Arm and Elbow Rash GuideTorso Rash
Common Causes
- Pityriasis rosea (Christmas-tree pattern)
- Heat rash (miliaria)
- Drug rash (begins on trunk)
- Shingles (follows one side of torso)
- Tinea versicolor
Diagnostic Clue
A rash that starts on the trunk and spreads outward, accompanied by recent medication use, is classic for a drug hypersensitivity reaction.
Drug-Induced RashesLeg Rash
Common Causes
- Cellulitis (lower leg)
- Varicose eczema / venous stasis
- Psoriasis (knees)
- Folliculitis (thighs)
- Leukocytoclastic vasculitis (palpable purpura)
Diagnostic Clue
Palpable purple bumps (purpura) on the lower legs — especially if non-blanching — can indicate vasculitis and require urgent evaluation.
Leg Rash Causes and TreatmentsGroin Rash
Common Causes
- Tinea cruris (jock itch)
- Candidal intertrigo
- Inverse psoriasis
- Contact dermatitis (from laundry products)
- Hidradenitis suppurativa
Diagnostic Clue
A red, scaly, well-bordered rash in the groin with an advancing edge is classic tinea cruris (jock itch) — responds well to OTC antifungal creams.
Groin Rash and Fungal InfectionsEmergency Rash Warning Signs
The following rash symptoms require immediate emergency medical attention. Do not wait to see if they improve on their own. Call emergency services or go to the nearest emergency department.
Purple or Red Non-Blanching Rash
Press a glass against the spots. If they do not turn white (blanch), this may indicate meningococcemia — a life-threatening bacterial infection of the blood. Call emergency services immediately. Every minute matters.
Call 999/911 NOWSudden Swelling of Face, Lips, or Throat
Angioedema affecting the throat can block the airway within minutes. Use epinephrine (EpiPen) if prescribed. Even if symptoms seem to improve after antihistamine, seek emergency care — swelling can rebound.
Epinephrine + 999/911Rash with Difficulty Breathing or Wheezing
Respiratory compromise alongside a rash indicates anaphylaxis — a systemic allergic emergency requiring epinephrine, oxygen, and IV treatment. Antihistamines alone are not adequate for anaphylaxis.
Call 999/911 NOWWidespread Blistering After New Medication
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are rare but life-threatening drug reactions causing skin to peel in sheets. Stop the medication immediately and seek emergency burn-unit care.
Emergency DepartmentRash with Very High Fever (39°C / 102°F+)
High fever combined with rash suggests a serious systemic infection — scarlet fever, Rocky Mountain spotted fever, bacterial sepsis, or DRESS syndrome. Do not manage at home with paracetamol alone.
Same-day emergency careRapid Skin Spreading Over Hours
Cellulitis that expands its borders over hours, or a rash that covers new body areas rapidly, indicates an aggressive infectious or immune process. Mark the border and monitor every 2 hours — escalate to emergency care if expansion continues.
Same-day emergency carePrevention Tips for Rash Symptom Triggers
Many rash symptoms are preventable with targeted lifestyle strategies. Understanding your personal triggers and building protective habits reduces both flare frequency and severity.
Identify and avoid contact allergens
Common triggers include nickel, fragrances, latex, and preservatives. Patch testing by a dermatologist pinpoints your specific sensitivities.
Maintain a strong skin barrier
Daily moisturizing with fragrance-free emollients (ceramide-based) significantly reduces eczema flares and prevents irritant rashes.
Manage heat and sweat
Wear breathable, loose-fitting natural fabrics in hot weather. Shower promptly after sweating to prevent heat rash and folliculitis.
Practice hand hygiene
Many contagious rashes — impetigo, ringworm, scabies — spread via direct contact. Regular handwashing breaks the transmission chain.
Keep vaccinations current
Vaccines for chickenpox, measles, and shingles (Shingrix for adults 50+) prevent major viral exanthem illnesses entirely.
Manage stress actively
Stress is a proven trigger for eczema, psoriasis, and hives flares. Regular exercise, adequate sleep, and mindfulness practices reduce inflammatory flares.
Frequently Asked Questions
Expert answers to the most searched rash symptom questions.
Continue Learning About Rashes
Medical Disclaimer: The symptom descriptions, severity assessments, and recommendations on this page are for educational purposes only and do not constitute medical advice, diagnosis, or treatment. Rash symptoms vary significantly across individuals and conditions. Always seek the advice of a qualified dermatologist or physician for any skin condition. In a medical emergency, call your local emergency services immediately. Read our full medical disclaimer.