Rash with Blisters: Causes, Diagnosis, and When to Seek Help
Medically Reviewed By
Dr. Marcus Chen, FAAD
Last Updated
January 19, 2026
A rash with blisters (vesicles or bullae) narrows the diagnostic possibilities significantly compared to a simple itchy red rash. Blisters form when fluid accumulates either within the epidermis (intraepidermal — smaller, more fragile vesicles, as in chickenpox) or at the dermo-epidermal junction (subepidermal — larger, tenser bullae, as in bullous pemphigoid). This distinction — vesicles versus bullae — is the first diagnostic branch point. The next most important questions are: Which body area is affected? (Chickenpox: widespread everywhere; shingles: one-sided dermatomal band; dyshidrotic eczema: palms and finger sides; herpes simplex: lip border or genitals.) Is the blistering accompanied by pain or itch? (Shingles and herpes: burning pain; eczema blisters: intense itch; pemphigoid: intense itch before blisters form.) Is mucosal involvement present? (Mouth, eyes, genitals involved — SJS: emergency; erythema multiforme; pemphigoid.) Has a new medication been started? (SJS/TEN within 7–14 days of a new drug — emergency.) Blistering rashes span the spectrum from entirely benign and common (dyshidrotic eczema, chickenpox in healthy children) to severe emergencies (toxic epidermal necrolysis, neonatal herpes, necrotizing skin infections) — this guide helps navigate that range.
Quick Medical Summary
Possible Causes of Blistering Rash: Ranked and Characterized
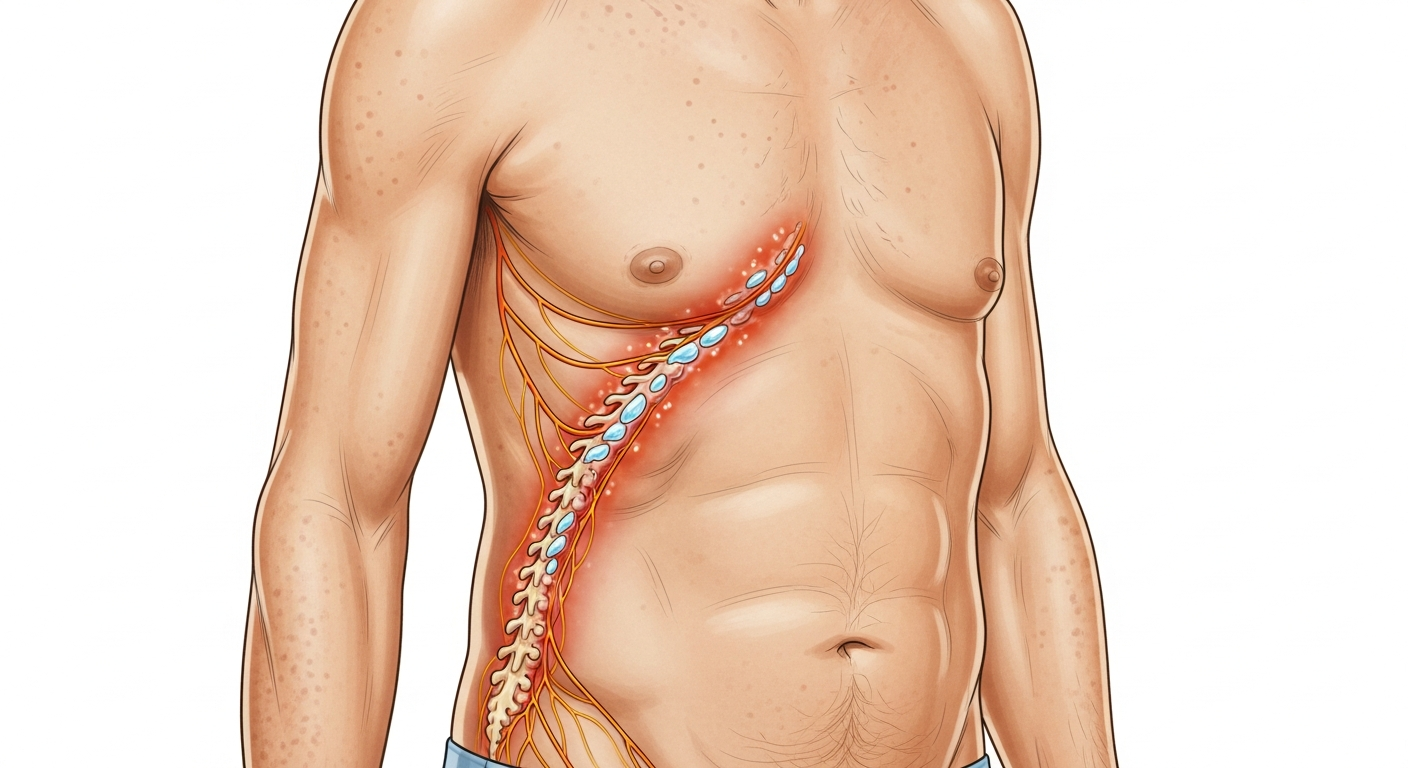
Chickenpox (varicella) is the most recognizable blistering rash in children — intensely itchy vesicles with the pathognomonic 'dewdrop on a rose petal' appearance (clear, teardrop vesicle on a red base), appearing in successive crops over 3–7 days, in all stages simultaneously (macule, papule, vesicle, pustule, crust), distributed across the trunk and scalp and spreading to the face and extremities. It is the prototypical intraepidermal vesicular rash. The virus spreads by respiratory droplets and direct contact with lesion fluid; contagious until all lesions are fully crusted. Shingles (herpes zoster) produces grouped vesicles in a unilateral dermatomal distribution — the same side of the body, in the shape of the nerve root territory, from the spine curving around to the midline at the front. It never crosses the midline. Intense burning pain precedes the rash by 1–3 days. Herpes simplex (HSV-1 and HSV-2) produces grouped vesicles on a red base — HSV-1 on the lip border (cold sores), HSV-2 in the genital area — in the same location each recurrence, with a prodrome of tingling or burning 1–2 days before the blisters appear. Dyshidrotic eczema (pompholyx) produces intensely itchy, small, deep-seated vesicles along the lateral sides of the fingers and on the palms and soles — they look like 'tapioca pearls' under the skin surface, are not fragile, and dry and peel over 2–4 weeks. Allergic contact dermatitis in acute form produces weeping vesicles and bullae in the exact location and shape of the allergen contact — linear blistering streaks from poison ivy contact are classic. Bullous pemphigoid produces large, tense (difficult to rupture) bullae on inflamed or normal-appearing skin of the elderly, preceded by intensely itchy urticarial lesions — an autoimmune condition. Impetigo (bullous type) from Staphylococcus aureus produces large fragile blisters (2–3cm) with thin roofs that rupture easily, leaving honey-colored crusts. Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis: blistering beginning with target-like lesions on the trunk, spreading to mucosal surfaces (mouth, eyes, genitals) — a drug reaction emergency.
How to Narrow Down the Diagnosis of Blistering Rash
Blister size is the first discriminating feature. Vesicles (small, 1–5mm): chickenpox (multiple stages simultaneously), herpes simplex (grouped on red base), herpes zoster (grouped, dermatomal), dyshidrotic eczema (deep-seated, palms/finger sides), early SJS. Bullae (large, >5mm): bullous pemphigoid (large tense — very difficult to rupture), bullous impetigo (thin-roofed, rupture easily), allergic contact dermatitis (fluid-filled, tense), bullous erysipelas, diabetic bullae, SJS/TEN (spreading large areas of skin loss). Distribution: Bilateral symmetric hands/feet: dyshidrotic eczema. Widespread with all stages simultaneously: chickenpox. Strictly one-sided dermatomal band: herpes zoster. Same spot, recurring: herpes simplex. In allergen contact shape: allergic contact dermatitis. Elderly, on trunk and limbs: bullous pemphigoid. Neonatal (newborn): neonatal HSV, SSSS, or epidermolysis bullosa. Age of the patient: children → chickenpox, bullous impetigo, SSSS. Young adults → herpes simplex, dyshidrotic eczema, allergic contact dermatitis. Older adults → herpes zoster (shingles), bullous pemphigoid. Mucosal involvement (mouth/eyes/genitals): Stevens-Johnson Syndrome if drug-associated; erythema multiforme major if post-herpes; pemphigus vulgaris (autoimmune — painful oral erosions often precede skin blisters). The Nikolsky sign — gentle lateral pressure on normal-appearing skin produces skin separation (peeling off in sheets): positive in SJS/TEN, SSSS, pemphigus vulgaris; negative in bullous pemphigoid. This test, performed by a clinician, immediately distinguishes the life-threatening blistering conditions from benign ones.
When Blistering Rash Becomes Serious: Red Flags and Emergency Signs
Most blistering rashes are uncomfortable but not life-threatening. The following require emergency or urgent evaluation. Blistering rash involving the mouth, eyes, or genitals after starting a new medication: Stevens-Johnson Syndrome — stop ALL medications that could be causative, go to the emergency department immediately. SJS progresses rapidly to TEN (toxic epidermal necrolysis) with massive skin loss resembling a severe burn — mortality in TEN can exceed 30%. Blistering rash in a newborn under 4 weeks of age: neonatal herpes simplex (HSV) — acquired during delivery, can disseminate to the brain and organs — requires emergency IV aciclovir treatment without delay. A widespread, peeling blistering rash in a young child with fever: staphylococcal scalded skin syndrome (SSSS) — staphylococcal toxin causes superficial skin peeling, the Nikolsky sign is positive, and IV antibiotics are needed. Rapidly expanding blistering skin with extreme pain, fever, and systemic toxicity: necrotizing fasciitis — the pain is disproportionate to appearance and comes from deeper tissue destruction. This is a surgical emergency with high mortality. Blistering shingles on the face involving the nose tip (Hutchinson's sign — nasolacrimal branch): high risk of ocular shingles (herpes zoster ophthalmicus) causing uveitis and permanent vision loss — same-day ophthalmology. Bullous pemphigoid in an elderly patient covering large body areas: requires systemic immunosuppression and wound care — hospitalization may be needed for widespread disease or secondary infection. Blistering rash with non-healing, raw areas in an elderly patient with worsening confusion: possible paraneoplastic pemphigus or severe drug reaction — requires urgent dermatology and oncology evaluation.
Key Symptoms
- Itchy vesicles in all stages simultaneously, widespread (chickenpox)
- Grouped vesicles on one side of body, preceded by burning pain (shingles)
- Deep-seated vesicles on palms and finger sides, intensely itchy (dyshidrotic eczema)
- Small grouped blisters recurring on lip border or genitals (herpes simplex)
- Large tense bullae on elderly trunk with preceding intense itch (bullous pemphigoid)
- Large fragile blisters rupturing to honey crusts (bullous impetigo)
- Blistering in exact pattern of allergen contact, acute onset (allergic contact dermatitis)
- Blistering of mouth, eyes, genitals with skin detachment after new drug (SJS — emergency)
Treatment Options
- Chickenpox: calamine lotion; antihistamines; aciclovir for high-risk patients
- Shingles: valaciclovir within 72h; ophthalmology same day if facial/eye involvement
- Dyshidrotic eczema: potent topical steroid; emollient; nickel avoidance; dupilumab
- Herpes simplex: topical or oral aciclovir; valaciclovir for episodic or suppressive
- Bullous pemphigoid: clobetasol 0.05%; systemic steroids + steroid-sparing agents
- Bullous impetigo: oral antibiotics; wound care
- Allergic contact dermatitis: remove allergen; oral prednisolone for severe blistering
- SJS/TEN: emergency hospitalization; stop causative drug; burns-unit supportive care
| Condition | Blister Type | Distribution | Emergency? |
|---|---|---|---|
| Chickenpox | Small vesicles — all stages | Widespread, trunk first | No — manage symptoms |
| Shingles | Grouped vesicles | Unilateral dermatomal band | Antiviral within 72h; ophtho if facial |
| Herpes Simplex | Small grouped vesicles | Lip border or genitals, recurring | No — antiviral treatment |
| Dyshidrotic Eczema | Deep-seated vesicles | Palms, finger sides, soles | No — topical treatment |
| Bullous Pemphigoid | Large tense bullae | Trunk and limbs, elderly | Urgent dermatology referral |
| SJS/TEN | Large coalescing + skin loss | Widespread + mucosal | YES — emergency immediately |
Narrow Down Your Diagnosis Further
When to See a Doctor Immediately
- Difficulty breathing or swallowing
- Swelling of the face, lips, or tongue
- High fever or severe chills
- Rapid spreading over a large body surface area
- Extreme pain, dizziness, or confusion
Frequently Asked Questions
Disclaimer
The medical information provided in this article is for educational purposes only and should not replace professional medical advice, diagnosis, or treatment. Always consult with a board-certified dermatologist or primary care physician regarding any severe or persistent skin conditions.