Painful Rash: Causes, Diagnosis, and When to Seek Emergency Care
Medically Reviewed By
Dr. Marcus Chen, FAAD
Last Updated
October 14, 2025
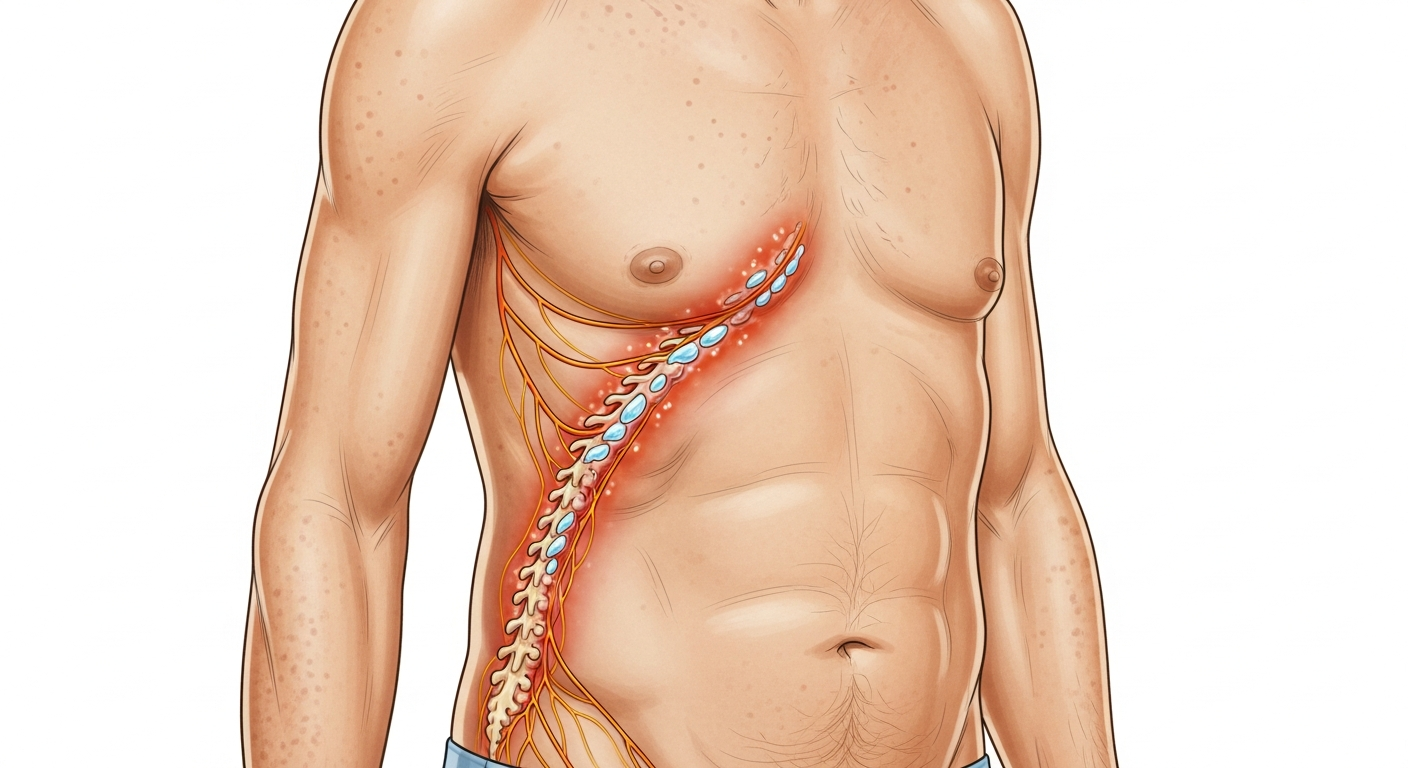
Pain is not the usual primary symptom of most rashes — itch is far more common. When a rash is painful rather than (or in addition to) itchy, it points toward a significantly narrowed differential diagnosis, several of which are medically serious. The most important painful rash not to miss is shingles (herpes zoster), where burning, shooting, or aching pain on one side of the body — often severe enough to be confused with cardiac, pleural, or abdominal pain — precedes the rash by 1–3 days and allows antiviral treatment to be started before the rash appears. Cellulitis is painful (tender to touch) and requires antibiotic treatment. Erythema nodosum causes exquisitely tender deep nodules on the shins. Necrotizing fasciitis — a rare but life-threatening bacterial skin infection — presents with extreme, disproportionate pain before the skin appearance becomes alarming: the pain far exceeds what the skin surface shows, because the bacteria are destroying the deeper tissue layers. This guide covers the important causes of painful rash, how to distinguish them, and the critical warning features that indicate emergency care is needed.
Quick Medical Summary
Causes of Painful Rash: Ranked by Clinical Importance
Shingles (herpes zoster) is the most common cause of a significantly painful rash in adults. The pain precedes skin changes by 1–3 days — burning, aching, electric-shock quality pain on one side of the body (chest, back, face, or limb) in the distribution of a single nerve root, sometimes severe enough to simulate a cardiac event (left chest herpes zoster), pleurisy (intercostal herpes zoster), or appendicitis (lumbar herpes zoster). When the skin changes appear — grouped vesicles in a dermatomal band — the diagnosis becomes clear. Starting antiviral treatment (valaciclovir 1g three times daily for 7 days) within 72 hours of rash onset is critical: it reduces the risk of post-herpetic neuralgia (PHN) — chronic, debilitating neuropathic pain persisting months to years — particularly in elderly patients. Cellulitis is painful by its nature: the rapidly expanding bacterial infection in the skin and subcutaneous tissue produces intense tenderness at the affected area (typically the lower leg) that increases with gentle palpation and is disproportionately tender compared to the surface appearance. Erythema nodosum produces exquisitely tender, deep, painful red or violet nodules (2–5cm) on the fronts of the shins — the tenderness is deep (nodules sit in the fat layer), and the overlying skin may be only mildly red. It is a reactive condition from underlying illness (streptococcal infection, IBD, sarcoidosis, pregnancy, medications). Painful blistering rash on the hand or arm from an industrial chemical, strong acid/alkali, cement (chromate), or hot liquid: chemical or thermal burn-pattern contact injury, distinguishable by the exposure history. Contact dermatitis from extreme exposures (phytophotodermatitis from giant hogweed sap + UV) can produce severe, burning, blistering, painful rash in the exact pattern of sap contact. Pyoderma gangrenosum is an intensely painful, rapidly enlarging ulcer with a violaceous (purple) undermined border — not infectious, but inflammatory — associated with IBD, rheumatoid arthritis, and monoclonal gammopathy.
How to Distinguish the Causes of Painful Rash
The character of the pain is the most discriminating diagnostic feature. Burning, electric-shock, dermatomal, one-sided: shingles — the nerve pain of herpes zoster is highly characteristic (neuropathic). Seek antiviral treatment immediately if within 72 hours of rash onset. Deep, exquisite tenderness on the shins in discrete nodules: erythema nodosum — requires investigation of underlying cause. Expanding tenderness from a skin wound with warmth and swelling: cellulitis — requires antibiotics. Extreme, disproportionate pain with minimal skin changes in a systemically unwell patient: necrotizing fasciitis until proven otherwise — emergency surgery. Burning pain in an exact area matching a chemical, plant, or thermal exposure: contact or phototoxic burn. The location of the painful rash provides additional diagnostic clarity. One-sided dermatomal band: shingles — the only common rash with severe burning neuropathic pain in a dermatomal pattern. Front of shins (bilateral or unilateral): erythema nodosum — deep tender nodules. Lower leg, from a wound: cellulitis. Genital area: primary genital herpes (HSV-2 first episode is exquisitely painful, distinguishing it from recurrent episodes which are milder), or Bartholin's abscess. Anywhere, expanding rapidly: necrotizing fasciitis — assess with fingertip pressure along the wound border for the 'finger test' (used surgically). Oral mucosa or genital mucosa: herpes simplex, Stevens-Johnson Syndrome, or pemphigus vulgaris. Timing is also useful: pain before rash by days → shingles; pain simultaneous with rash → cellulitis, erythema nodosum, contact burn; pain after rash appearance → post-herpetic neuralgia from previous shingles.
Emergency Warning Signs: When Painful Rash Requires Emergency Care
The painful rash that demands emergency services or an emergency department visit follows specific patterns. Extreme pain with a skin wound or rash that seems disproportionate to the surface appearance, with systemic toxicity, fever, and rapid deterioration: necrotizing fasciitis — bacteria (typically Streptococcus, Staphylococcus, polymicrobial) are destroying fascia and deeper tissue far beyond what the skin surface reveals. Surgery (extensive debridement) is the only cure; delay of even hours dramatically increases mortality. Do not wait for the skin to look 'bad enough.' Pain, swelling, redness, and fever from a hand wound, finger bite, or puncture injury: flexor tenosynovitis or necrotizing hand infection — the enclosed anatomy of the hand allows infection to track rapidly through tendon sheaths, and these are orthopedic/surgical emergencies. Severe burning pain on the face following a dermatomal distribution, with rash appearing on the nose tip or periocular skin: herpes zoster ophthalmicus — same-day ophthalmology evaluation alongside antivirals, as corneal involvement can rapidly cause permanent vision loss. Rapidly spreading painful cellulitis that does not improve within 12–24 hours of starting appropriate antibiotics: resistant organism, deep infection, or fascial involvement — escalate to emergency evaluation. Intensely painful ulcer with violaceous border expanding despite wound care in a patient with IBD or rheumatoid arthritis: pyoderma gangrenosum — this is crucially an inflammatory, not infectious, ulcer; surgical debridement worsens it dramatically (pathergy); it requires systemic immunosuppression (prednisolone, cyclosporin). Alert the surgical team before any debridement of suspected pyoderma gangrenosum. Painful blistering rash in a neonate or immunocompromised patient: potential HSV or VZV dissemination — emergency IV antiviral treatment.
Key Symptoms
- Burning/electric-shock pain on one body side, before rash appears (pre-shingles neuralgia)
- Grouped vesicles in one-sided dermatomal band with burning pain (shingles)
- Expanding warmth, tenderness, and swelling from a wound with fever (cellulitis)
- Deep tender red nodules on front of shins (erythema nodosum)
- Extreme pain disproportionate to skin appearance with systemic toxicity (necrotizing fasciitis — emergency)
- Burning blistering rash in exact plant-sap or chemical contact pattern (contact burn)
- Intensely painful ulcer with violaceous border expanding despite wound care (pyoderma gangrenosum)
- Painful blistering rash on face near eye with burning (herpes zoster ophthalmicus — ophtho emergency)
Treatment Options
- Shingles: valaciclovir 1g 3× daily for 7 days — within 72 hours of rash onset
- Post-herpetic neuralgia: gabapentin; pregabalin; amitriptyline; topical lidocaine patch
- Cellulitis: flucloxacillin or cephalexin; IV antibiotics if spreading or febrile
- Erythema nodosum: NSAIDs; leg elevation; treat underlying cause; prednisolone if severe
- Necrotizing fasciitis: emergency surgery + IV broad-spectrum antibiotics — do not delay
- Phototoxic/chemical burn: remove from exposure; cool water; wound care; steroids
- Pyoderma gangrenosum: prednisolone or cyclosporin — do NOT surgically debride
- Herpes zoster ophthalmicus: antiviral + same-day ophthalmology — corneal protection
| Condition | Character of Pain | Location | Emergency? |
|---|---|---|---|
| Shingles | Burning/neuropathic, pre-rash | Unilateral dermatomal band | Antiviral within 72h; ophtho if facial |
| Cellulitis | Tenderness, expanding | From wound outward | Same day — antibiotics |
| Erythema Nodosum | Deep tender nodules | Front of shins | GP evaluation; investigate cause |
| Necrotizing Fasciitis | Extreme, disproportionate to appearance | Anywhere — rapidly spreading | EMERGENCY — surgery now |
| Pyoderma Gangrenosum | Intensely painful ulcer | Any — often leg, abdomen | Urgent — do NOT debride; immunosuppression |
| HZ Ophthalmicus | Burning, periocular + nose tip | Face — trigeminal nerve | Antiviral + same-day ophthalmology |
Narrow Down Your Diagnosis Further
When to See a Doctor Immediately
- Difficulty breathing or swallowing
- Swelling of the face, lips, or tongue
- High fever or severe chills
- Rapid spreading over a large body surface area
- Extreme pain, dizziness, or confusion
Frequently Asked Questions
Disclaimer
The medical information provided in this article is for educational purposes only and should not replace professional medical advice, diagnosis, or treatment. Always consult with a board-certified dermatologist or primary care physician regarding any severe or persistent skin conditions.