What Causes a Rash on the Chest?
Medically Reviewed By
Dr. Marcus Chen, FAAD
Last Updated
March 13, 2026
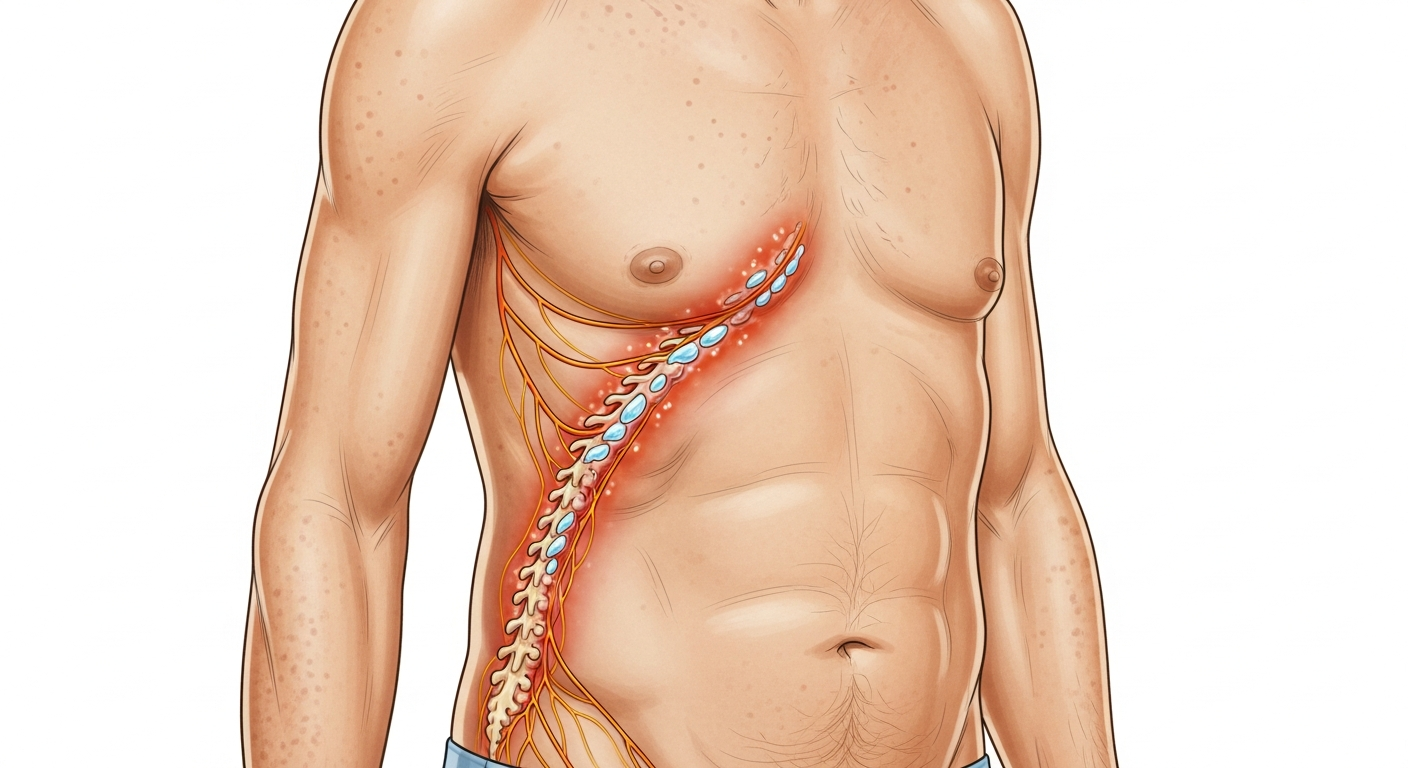
The chest is a common location for skin rashes because it is a sun-exposed area, a frequent contact site for jewelry and fabric, an area where sweat accumulates, and the starting point for many viral and drug-related rashes that begin centrally and spread outward. Common causes of chest rash include shingles (herpes zoster — typically unilateral, following a dermatomal band across one side of the chest), pityriasis rosea (oval scaly patches in a 'Christmas tree' pattern along the lines of skin cleavage), seborrheic dermatitis (yellowish flaking rash on the central chest), heat rash (miliaria — small red bumps in the décolletage and skin folds), contact dermatitis from necklaces, bra fabric, or sunscreen, polymorphic light eruption from sun exposure, and viral exanthems that begin on the trunk. Shingles is worth highlighting: it causes severe burning pain before the rash appears, and the unilateral, band-like distribution is pathognomonic — early antiviral treatment within 72 hours of rash onset significantly reduces severity and prevents long-term nerve pain.
Quick Medical Summary
Shingles, Pityriasis Rosea, and Seborrheic Dermatitis
Shingles (herpes zoster) on the chest is one of the most important diagnoses not to miss. It presents as severe burning, shooting, or stabbing pain on one side of the chest 1–3 days before any skin changes. When the rash appears, it is unilateral (one side only), follows the dermatome of the affected thoracic nerve root (a band from the spine around one side to the midline of the chest), and produces grouped vesicles (blisters) on a red base. The unilateral, dermatomal, painful blistering rash is highly characteristic. Start antiviral therapy (aciclovir 800mg 5×/day, or valaciclovir 1g 3×/day) within 72 hours of rash onset to reduce severity and the risk of post-herpetic neuralgia (chronic nerve pain lasting months to years in the rash distribution). Pityriasis rosea begins with a single large 'herald patch' on the chest or back — a solitary, oval, slightly scaly pink patch 2–5 cm diameter. Within 1–2 weeks, numerous smaller similar patches spread across the trunk in a 'Christmas tree' pattern (parallel to the skin cleavage lines, angled diagonally across the back). It is mildly itchy and self-limiting, resolving within 6–12 weeks. Seborrheic dermatitis on the chest produces yellowish-white greasy scale on the central upper chest (between the nipples and below the sternal notch) — mirroring its distribution on the scalp, eyebrows, and nose creases. It responds to topical ketoconazole or zinc pyrithione shampoo used as a body wash.
Heat Rash, Contact Dermatitis, and Viral Rash on the Chest
Heat rash (miliaria rubra) on the chest typically affects the décolletage, under the breasts, and the inframammary fold (skin under the breast) — areas where fabric presses against skin and sweat cannot evaporate. The rash consists of tiny red papules and vesicles with a prickling or burning quality. Cooling the environment, removing tight or synthetic fabric, and applying calamine lotion resolves most heat rash within 3–4 days. Contact dermatitis on the chest has characteristic shapes: a rectangular or chain-shaped rash from a necklace or pendant (matching the jewelry exactly); a bra-strap-shaped rash from rubber or elastic; a band of rash across the chest from a bra underwire. Common chest allergens include nickel (in jewelry clasps and costume jewelry), rubber in bra elastic, formaldehyde from fabric finishes, and fragrance in body lotion or perfume. Viral exanthems — roseola, measles, rubella, drug rashes — typically begin on the trunk (chest and abdomen) and spread outward. The chest and abdomen are usually the most densely affected areas. These morbilliform (measles-like) rashes are flat or slightly raised, pink-to-red spots covering large areas without the specific patterning of pityriasis rosea or seborrheic dermatitis.
Acne, Folliculitis, and Sun-Related Chest Rashes
Chest acne (truncal acne) produces comedones (blackheads and whiteheads), papules, and pustules on the chest and upper back — driven by sebaceous gland activity, Cutibacterium acnes colonization, and hormonal influences. It is treated with topical benzoyl peroxide, retinoids, or salicylic acid, and for moderate-to-severe cases, oral antibiotics or isotretinoin. Folliculitis from hot tub use (Pseudomonas folliculitis) produces a distinctive rash: intensely itchy red papules and pustules around hair follicles on the trunk, appearing 12–48 hours after hot tub use in poorly maintained facilities. It resolves spontaneously within 5–10 days in most cases. Polymorphic light eruption (PLE) commonly affects the décolletage — the upper chest area exposed by low-cut clothing — producing itchy papules within hours of sun exposure in spring. Sun-protective clothing and broad-spectrum SPF 50+ sunscreen prevent PLE on the chest. Intertrigo (friction rash) beneath the breasts produces red, moist, burning skin in the inframammary fold, driven by moisture, warmth, and friction — treat with barrier creams, moisture-wicking fabric, and antifungal cream if candidal superinfection is present.
Key Symptoms
- Unilateral burning pain then blistering rash on one side of chest (shingles — urgent)
- Single large oval scaly patch followed by Christmas-tree pattern across trunk (pityriasis rosea)
- Yellowish flaking scale on central upper chest (seborrheic dermatitis)
- Tiny red prickly bumps in décolletage or under breasts in hot weather (heat rash)
- Rash matching necklace or bra strap shape exactly (contact dermatitis)
- Widespread pink-red spots on chest and trunk with or without fever (viral/drug rash)
Treatment Options
- Shingles: antiviral (valaciclovir) within 72 hours of rash onset — do not delay
- Pityriasis rosea: reassurance; antihistamines for itch; natural UVB light speeds resolution
- Seborrheic dermatitis: ketoconazole 2% cream or zinc pyrithione body wash
- Heat rash: cool environment, loose cotton clothing, calamine lotion
- Contact dermatitis: remove allergen, hydrocortisone cream, antihistamines
- Chest acne: benzoyl peroxide wash; topical retinoid; dermatologist for severe cases
When to See a Doctor Immediately
- Difficulty breathing or swallowing
- Swelling of the face, lips, or tongue
- High fever or severe chills
- Rapid spreading over a large body surface area
- Extreme pain, dizziness, or confusion
Frequently Asked Questions
Disclaimer
The medical information provided in this article is for educational purposes only and should not replace professional medical advice, diagnosis, or treatment. Always consult with a board-certified dermatologist or primary care physician regarding any severe or persistent skin conditions.