How to Tell If a Rash Is Serious
Medically Reviewed By
Dr. Marcus Chen, FAAD
Last Updated
February 21, 2026
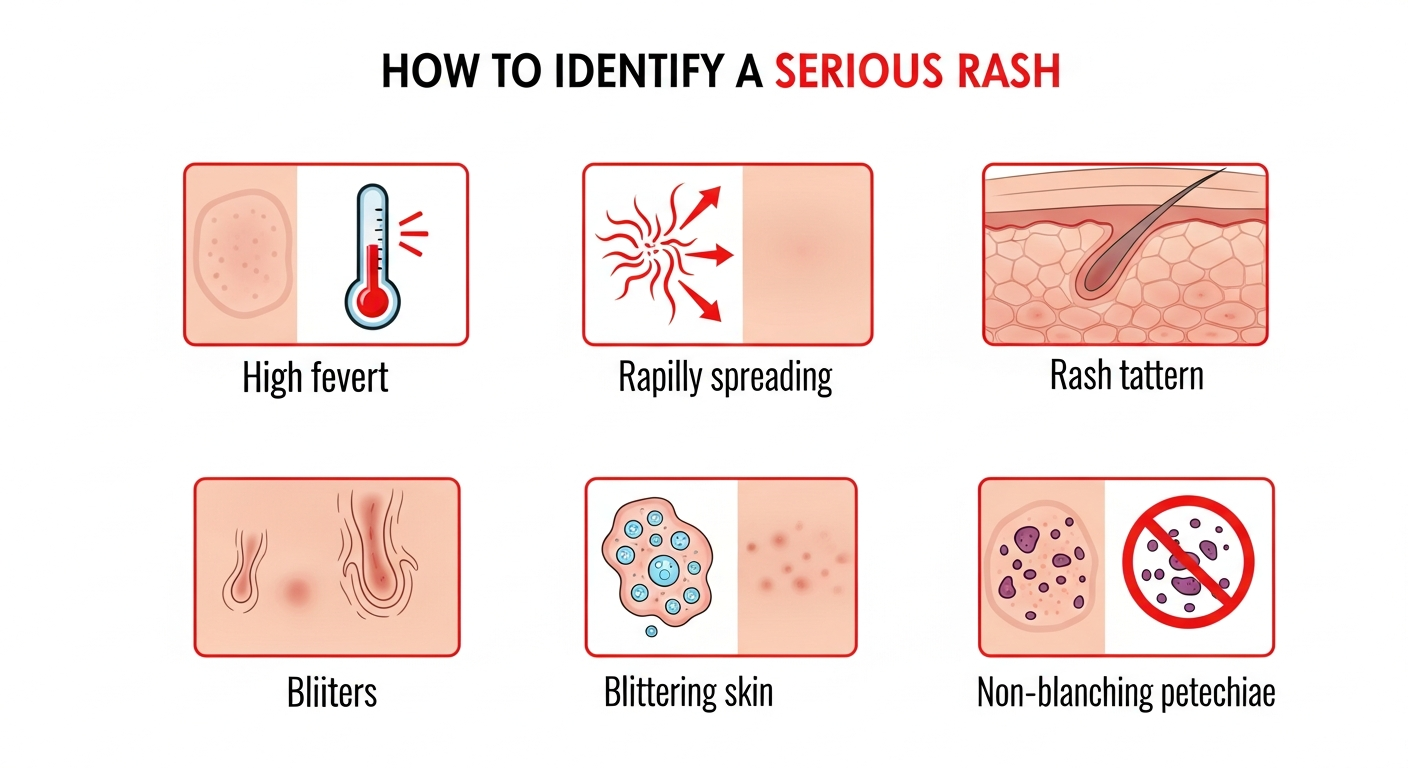
Most rashes are benign and self-limiting, but certain features mark a rash as potentially serious or life-threatening. The single most critical sign is a non-blanching rash — one that stays red or purple when you press on it. This indicates bleeding into the skin (petechiae or purpura) and can signal meningococcal disease, sepsis, or vasculitis — all medical emergencies. Other serious signs include rash accompanied by high fever, difficulty breathing, swelling of the face or throat, confusion, neck stiffness, or a rash that spreads rapidly across large areas of the body within hours. Stevens-Johnson Syndrome (SJS) — a severe drug reaction — begins with flu symptoms and a painful, blistering rash that causes the skin and mucous membranes to peel away. Toxic shock syndrome, Rocky Mountain Spotted Fever, and Kawasaki disease are other serious rash diagnoses that require urgent intervention. Learning to distinguish these from common, benign rashes can be life-saving.
Quick Medical Summary
The Blanching Test: The Most Important Assessment
The blanching test (glass test) is the single most important first evaluation for any rash. Press firmly on a small area of the rash with a clear glass or the pad of your finger. A benign rash — caused by blood vessel dilation from inflammation — will turn white (blanch) under pressure as the blood is temporarily pushed out of the dilated vessels. Release pressure and the redness returns. A non-blanching rash does not change color under pressure. This means blood has leaked out of damaged blood vessels into the surrounding skin — a process called purpura (large patches) or petechiae (pinpoint dots). Non-blanching rashes are caused by vasculitis (blood vessel inflammation), coagulation disorders, septicemia, meningococcal disease, or Henoch-Schönlein Purpura (IgA vasculitis). If any part of a rash is non-blanching, treat it as a medical emergency and call emergency services. Meningococcal disease can kill within 24 hours; early identification and antibiotic treatment are lifesaving. The glass test is especially critical in children with fever — a blanching pink rash with fever is likely viral; a non-blanching purple rash with fever may be meningococcal disease.
Warning Signs That Require Emergency Care
Beyond the blanching test, several other features signal an emergency. Rapidly spreading rash: if a rash spreads visibly across the body over minutes to hours, this suggests an acute systemic reaction — anaphylaxis, severe drug reaction, or rapidly spreading infection like necrotizing fasciitis. Facial or throat swelling accompanying any rash indicates anaphylaxis — the throat swelling can close the airway within minutes. Call emergency services and use epinephrine (EpiPen) if available. High fever (above 103°F / 39.4°C) combined with a rash significantly increases the probability of a serious infectious cause: scarlet fever, Rocky Mountain Spotted Fever, meningococcemia, toxic shock syndrome, or viral hemorrhagic fevers. Blistering rash over large body areas — especially involving the mouth, eyes, or genitals — suggests Stevens-Johnson Syndrome or Toxic Epidermal Necrolysis (TEN), both severe drug reactions with significant mortality. Painful rash: most inflammatory rashes itch rather than hurt. A painful rash — especially if accompanied by skin tenderness, warmth, and systemic illness — raises concern for cellulitis (spreading bacterial skin infection), necrotizing fasciitis (flesh-eating bacteria), or herpes zoster (shingles). Confusion or altered consciousness alongside any rash may indicate bacterial meningitis or toxic shock — both life-threatening.
Rashes That Can Wait vs. Rashes That Cannot
Many rashes are genuinely benign and simply need time and basic care. Contact dermatitis from a new soap, detergent, or plant (like poison ivy) causes intensely itchy, blistered rash in a pattern matching the exposure area — uncomfortable but not dangerous. Simple hives from a food trigger typically resolve within 24–48 hours with antihistamines and are only an emergency if the throat or tongue swells. Heat rash (miliaria) — tiny red bumps in skin folds after sweating — resolves within days with cooling. Eczema and psoriasis flares, while miserable, are not emergencies; they need routine dermatology care. Ringworm, despite its alarming name, is a common and easily treated fungal infection. Schedule a routine doctor appointment for: rashes that haven't improved after 2 weeks; rashes with no identifiable cause; rashes involving the face, eyes, or genitals; persistent itching interfering with sleep; or any rash in immunocompromised individuals. Go immediately to the emergency department for: non-blanching rash, rash with fever above 103°F, throat or tongue swelling, breathing difficulty, rapidly spreading rash, confusion, or large-area blistering.
Key Symptoms
- Non-blanching purple or red spots that stay colored under glass pressure (emergency)
- Rash spreading visibly across the body within hours (emergency)
- Facial, tongue, or throat swelling alongside any rash (emergency)
- Fever above 103°F (39.4°C) combined with a rash
- Large-area blistering affecting the mouth, eyes, or genitals
- Confusion, neck stiffness, or altered consciousness with a rash
Treatment Options
- For non-blanching rash: call emergency services immediately — do not wait
- For anaphylaxis signs: use epinephrine auto-injector and call emergency services
- For fever + rash: seek urgent medical evaluation same day
- For benign contact rash: cool compresses, hydrocortisone cream, antihistamines
- For hives: oral antihistamines; emergency care only if throat swells
- Routine appointment within a week for rashes that don't fit emergency criteria
When to See a Doctor Immediately
- Difficulty breathing or swallowing
- Swelling of the face, lips, or tongue
- High fever or severe chills
- Rapid spreading over a large body surface area
- Extreme pain, dizziness, or confusion
Frequently Asked Questions
Disclaimer
The medical information provided in this article is for educational purposes only and should not replace professional medical advice, diagnosis, or treatment. Always consult with a board-certified dermatologist or primary care physician regarding any severe or persistent skin conditions.