How to Stop a Rash from Itching
Medically Reviewed By
Dr. Marcus Chen, FAAD
Last Updated
February 28, 2026
Rash itching (pruritus) can be reduced quickly using a combination of cooling, antihistamines, topical treatments, and barrier protection. The fastest immediate relief comes from a cool compress or cool water — cold temperatures activate cold-sensitive nerve fibers that compete with and temporarily override itch signals (the same principle as rubbing a mosquito bite reduces the itch). Oral antihistamines (cetirizine, loratadine) block histamine receptors and are effective for allergic itch (hives, contact dermatitis, allergic eczema) within 1–2 hours. Hydrocortisone 1% cream reduces the underlying inflammation driving the itch and provides sustained relief over hours. For severe itch disrupting sleep, a brief course of sedating antihistamine (diphenhydramine — Benadryl) at night provides both itch relief and sedation, though tolerance develops quickly with nightly use. Understanding the mechanism of your specific rash itch helps choose the most targeted treatment — histamine-driven itch responds best to antihistamines, whereas nerve-mediated itch (in eczema and chronic kidney disease) may require different agents.
Quick Medical Summary
Fast Relief: Cooling, Antihistamines, and Topicals
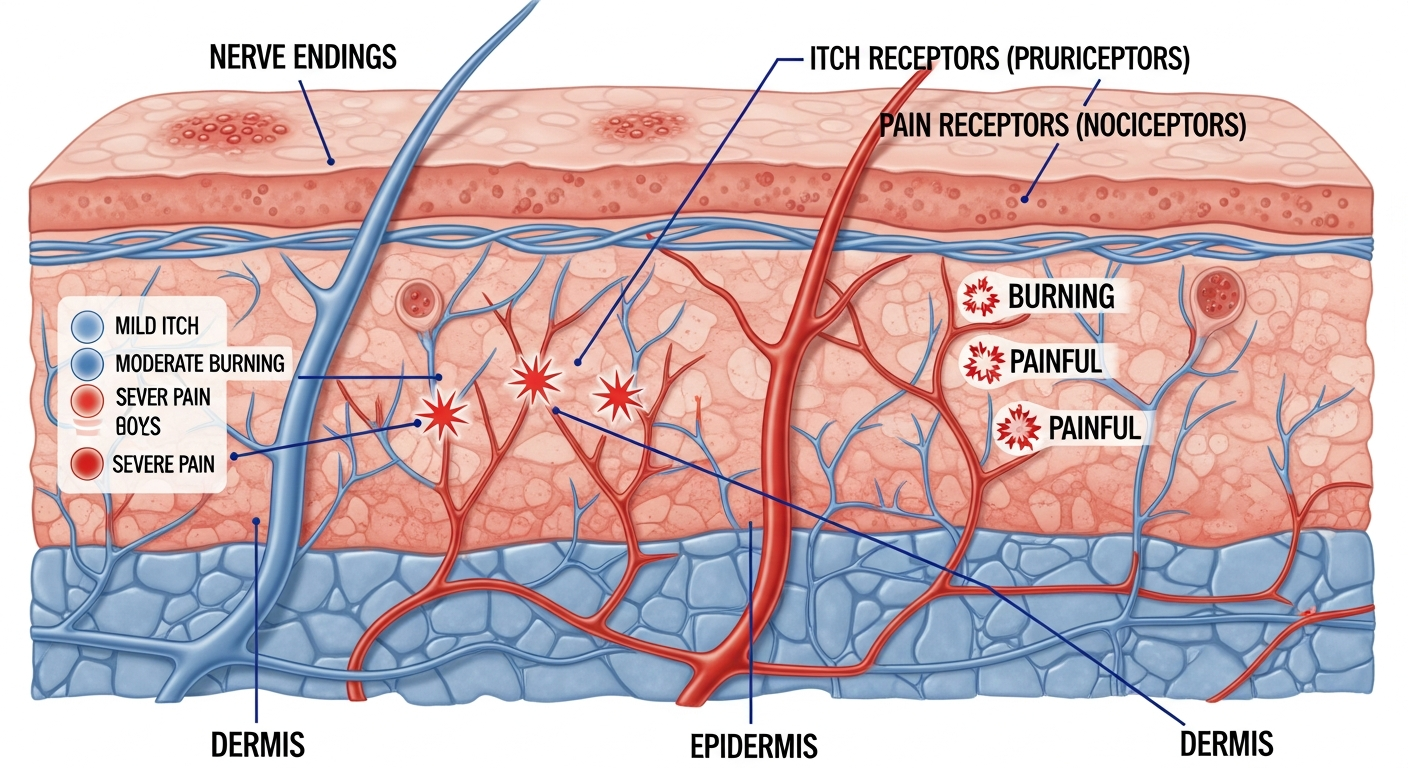
Cool compresses are the single fastest itch relief method available — apply a cool (not ice cold) damp cloth for 15–20 minutes; the cold activates TRPM8 receptors in skin nerve fibers that produce cooling sensation and directly inhibit itch-transmitting C-fibers. This provides immediate, if temporary, relief without any risk of side effects. Cold water showers achieve the same effect over larger areas. Oral antihistamines work within 1–2 hours and are most effective for histamine-driven itch: hives, contact dermatitis, insect bites, mild eczema. Second-generation non-sedating antihistamines (cetirizine 10mg, loratadine 10mg, fexofenadine 180mg) are preferred for daytime use — they do not impair cognitive function or driving ability. Cetirizine is generally the most potent. For nighttime use when sedation is acceptable, diphenhydramine 25–50mg or hydroxyzine 10–25mg provides both antihistamine effect and sedation. Topical hydrocortisone 1% cream provides sustained anti-inflammatory relief — apply a thin layer to the itchy rash twice daily for up to 7 days on body areas (3–5 days on the face). Stronger prescription topical steroids (betamethasone, clobetasol) are more effective for severely itchy conditions but require medical prescription.
Specific Treatments for Different Types of Itch
Eczema itch is incompletely relieved by antihistamines because much of the itch is histamine-independent — mediated by interleukin-31 (IL-31) and other cytokines. Dupilumab (Dupixent) — a biologic antibody targeting the IL-4/IL-13 pathway — dramatically reduces eczema itch within 2–4 weeks and is now the most effective treatment for moderate-to-severe atopic eczema itch. Topical calcineurin inhibitors (tacrolimus 0.03%/0.1%, pimecrolimus 1%) are steroid-free options that effectively suppress eczema itch, particularly on sensitive areas (face, eyelids, genitals) where steroids cause more side effects. Pramoxine 1% cream (a topical anesthetic) provides local itch relief for 30–60 minutes — available in AmLactin and Sarna lotion — useful as a bridge while other treatments take effect. Menthol 1–2% in aqueous cream or calamine provides cooling itch relief through TRPM8 receptor activation and is particularly useful for widespread itch. Colloidal oatmeal creams (Aveeno) have FDA-recognized skin-protective properties, reduce itch and erythema in eczema, and are safe for all ages. For nerve-mediated itch (neuropathic pruritus from postherpetic neuralgia or brachioradial pruritus), antihistamines are largely ineffective; gabapentin or pregabalin are more appropriate.
The Itch-Scratch Cycle and How to Break It
Scratching provides momentary relief by replacing the itch sensation with mild pain — this activates inhibitory neurons in the spinal cord that temporarily reduce itch transmission. However, scratching causes mechanical damage to the skin, releases more inflammatory mediators from mast cells, triggers more histamine release, and perpetuates the inflammatory cycle — making the itch worse overall, not better. The itch-scratch cycle is a pathological positive feedback loop that maintains itch long after the original trigger has resolved. Breaking this cycle requires both physical barrier measures and cognitive strategies. Physical barriers: wearing cotton gloves at night prevents unconscious nocturnal scratching; keeping fingernails trimmed short reduces trauma from scratching; applying cotton tubing (TubiGrip) over emollient-covered limbs in eczema reduces scratching damage. Habit reversal training (HRT) — a behavioral technique — teaches the patient to become aware of the impulse to scratch and substitute a competing response (pressing, pinching, applying cool compress). HRT has clinical evidence in eczema and chronic prurigo. The urge to scratch can also be partially satisfied by pressing firmly on the itchy area without the skin-breaking stroke of scratching, or applying light percussion (patting). Mindfulness meditation helps interrupt the anxiety-amplification of itch by reducing the emotional response to the itch sensation, effectively turning down the volume without eliminating the signal.
Key Symptoms
- Constant or episodic itching at the rash site, worse at night
- Scratch marks, excoriations, or broken skin from nocturnal scratching
- Localized itch at insect bite sites, hive locations, or rash patches
- Generalized body itch without visible rash (may indicate systemic cause)
- Burning or stinging in addition to itch (nerve-mediated types)
- Itch unresponsive to antihistamines (non-histamine-mediated eczema or neuropathic itch)
Treatment Options
- Cool compress 15–20 minutes — fastest immediate itch relief
- Oral antihistamines: cetirizine 10mg (best for daytime), diphenhydramine for nighttime
- Topical hydrocortisone 1% cream twice daily for up to 7 days
- Menthol 1% or calamine lotion for widespread, localized cooling effect
- Colloidal oatmeal bath or cream for widespread itch
- Prescription dupilumab or calcineurin inhibitors for eczema itch resistant to OTC treatment
When to See a Doctor Immediately
- Difficulty breathing or swallowing
- Swelling of the face, lips, or tongue
- High fever or severe chills
- Rapid spreading over a large body surface area
- Extreme pain, dizziness, or confusion
Frequently Asked Questions
Disclaimer
The medical information provided in this article is for educational purposes only and should not replace professional medical advice, diagnosis, or treatment. Always consult with a board-certified dermatologist or primary care physician regarding any severe or persistent skin conditions.