Difference Between Hives and a Rash
Medically Reviewed By
Dr. Marcus Chen, FAAD
Last Updated
December 11, 2025
Hives (urticaria) are a specific type of rash — but the two terms are not interchangeable. A rash is any change in skin color, texture, or appearance, and encompasses hundreds of distinct conditions. Hives are a precisely defined subset of rash characterized by three key features: (1) raised, pale-centered wheals surrounded by a red flare, (2) each individual wheal lasts fewer than 24 hours before fading (even as new ones appear elsewhere), and (3) intense itching is the dominant symptom. This migratory nature — lesions appearing and disappearing across the body — is diagnostic of urticaria and not seen in other rashes. Contact dermatitis, eczema, ringworm, and viral rashes do not migrate. Hives can occur anywhere on the body, whereas other rashes tend to affect specific characteristic locations. Treatment differs completely: hives respond quickly to antihistamines; most other rashes do not.
Quick Medical Summary
How to Identify Hives (Urticaria)
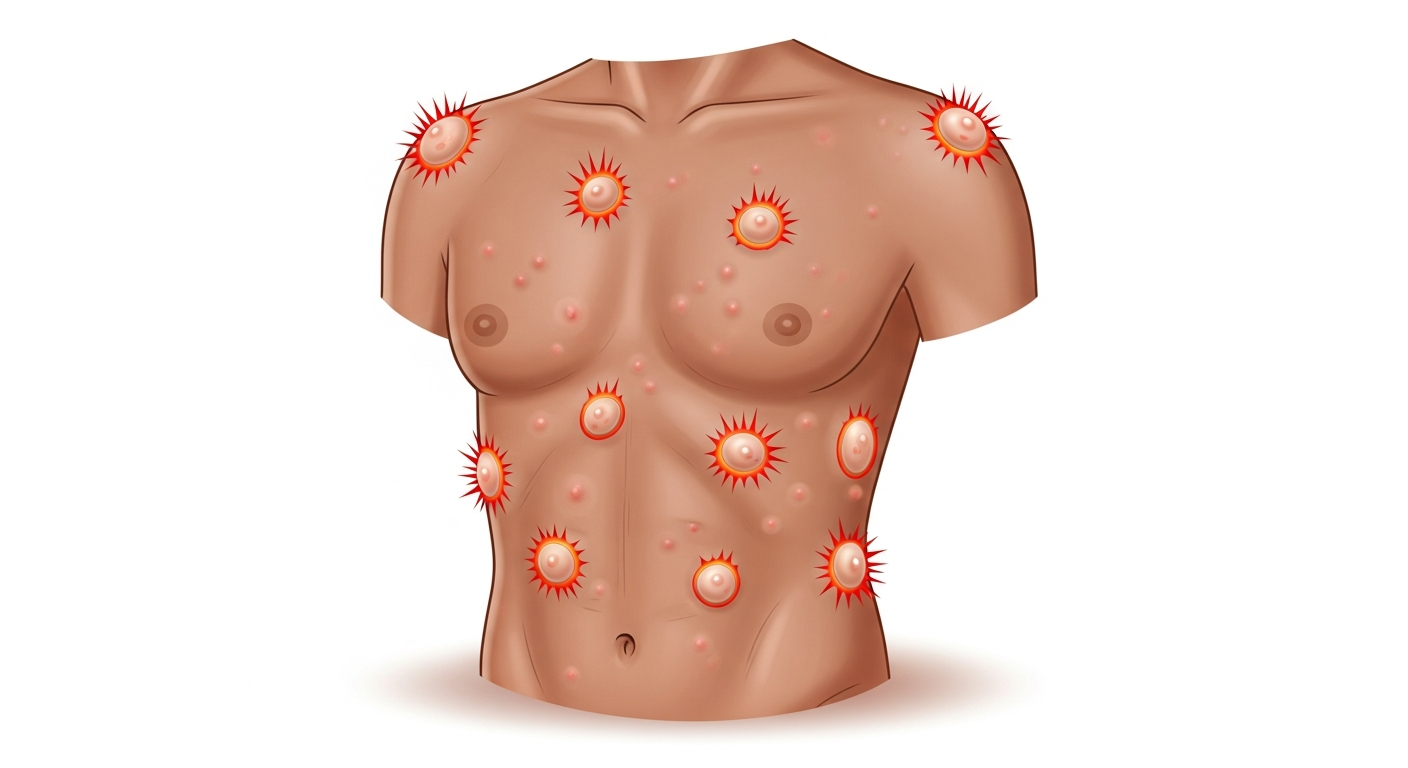
Urticaria produces wheals — circumscribed, edematous (swollen) plaques of the superficial dermis. Each wheal has three characteristic features that collectively distinguish it from all other rash types: (1) it is raised and palpable, with a pale, skin-colored or pink center and a surrounding red flare, (2) each individual lesion resolves completely within 24 hours (often within 30 minutes to a few hours), and (3) the itching is intense and often described as burning. This distinguishes hives from erythema (simple redness) which is flat and not raised. The temporary, migratory quality of hives is clinically pathognomonic: if the patient shows you a photo of red marks that are now gone, or new marks appearing in different areas each time they look, urticaria is the diagnosis. Hives can be triggered by food allergens, medications, infections, physical stimuli (cold, heat, pressure, vibration, sunlight), or occur spontaneously with no identifiable cause (chronic spontaneous urticaria). Angioedema — swelling of deeper skin and mucosal layers, affecting the lips, eyelids, tongue, and throat — accompanies urticaria in about 50% of cases. Angioedema without urticaria can be a sign of hereditary angioedema (HAE), a genetic complement deficiency requiring specialist management.
How Other Common Rashes Differ from Hives
Contact dermatitis: redness, blisters, and weeping confined to the exact area of allergen contact — it does not migrate, individual lesions last days to weeks (not hours), and is diagnosed by its contact-conforming shape. Antihistamines have modest benefit; topical corticosteroids are the primary treatment. Eczema (atopic dermatitis): chronic, relapsing, intensely itchy rash in skin folds — individual lesions are persistent (lasting weeks), with scaling, lichenification, and weeping that hives do not produce. Antihistamines have limited effectiveness for eczema. Psoriasis: well-defined, thick, silver-scaled plaques on elbows, knees, and scalp — permanent (not migratory), not intensely itchy, and unresponsive to antihistamines. Ringworm (tinea): ring-shaped, scaly patches that expand slowly over weeks — not migratory (the ring grows larger, not appearing and disappearing elsewhere), and treated with antifungals, not antihistamines. Viral exanthem: widespread, flat or slightly raised pink spots appearing suddenly with fever — do not migrate within 24 hours in the same way hives do, are not intensely itchy, and do not respond to antihistamines. Cellulitis: a bacterial skin infection — a single expanding area of warmth, redness, and swelling from an entry point — never migratory, very painful rather than itchy, and requires antibiotics.
Treatment: Hives vs. Other Rashes
Second-generation non-sedating H1 antihistamines are the cornerstone treatment for urticaria: cetirizine 10mg, loratadine 10mg, or fexofenadine 180mg once daily. These block H1 histamine receptors, preventing mast cell-derived histamine from producing wheals. For chronic spontaneous urticaria that doesn't respond to standard doses, doubling or quadrupling the cetirizine dose (off-label: up to 40mg/day) is supported by international guidelines. Omalizumab (anti-IgE biologic) is FDA-approved for chronic spontaneous urticaria unresponsive to antihistamines and produces remarkable clearance in 60–70% of patients. For anaphylaxis — urticaria with throat swelling, breathing difficulty, or cardiovascular collapse — epinephrine (EpiPen) is the life-saving treatment. Most non-urticarial rashes require different treatments: topical or systemic corticosteroids for eczema and contact dermatitis; antifungals for ringworm; antibiotics for bacterial infections; systemic medications for psoriasis. Using antihistamines for these non-urticarial rashes provides modest itch relief at best but does not treat the underlying condition.
Key Symptoms
- Hives: raised pale wheals with red flare, each lasting <24 hours, migrating to new areas
- Hives: intense itching, possibly burning sensation at each wheal location
- Other rash: lesions stay in the same location for days to weeks (not migratory)
- Other rash: scaling, crusting, lichenification, or blistering not seen in simple hives
- Angioedema with hives: swelling of lips, eyes, tongue — possible emergency if throat swells
- Contact rash: redness confined exactly to contact area (not migratory)
Treatment Options
- Hives: oral cetirizine 10mg, loratadine 10mg, or fexofenadine 180mg — first line
- Severe hives: higher-dose antihistamines; oral corticosteroid short course
- Chronic urticaria (>6 weeks): omalizumab (Xolair) via allergy specialist
- Anaphylaxis with hives: epinephrine auto-injector immediately, then emergency services
- Contact dermatitis rash: topical corticosteroid, not antihistamine alone
- Eczema: emollients, topical steroids, calcineurin inhibitors
When to See a Doctor Immediately
- Difficulty breathing or swallowing
- Swelling of the face, lips, or tongue
- High fever or severe chills
- Rapid spreading over a large body surface area
- Extreme pain, dizziness, or confusion
Frequently Asked Questions
Disclaimer
The medical information provided in this article is for educational purposes only and should not replace professional medical advice, diagnosis, or treatment. Always consult with a board-certified dermatologist or primary care physician regarding any severe or persistent skin conditions.