Can Sunburn Cause a Rash?
Medically Reviewed By
Dr. Marcus Chen, FAAD
Last Updated
November 27, 2025
Yes — sun exposure causes several distinct types of rash beyond simple sunburn. Sunburn itself is a radiation-induced inflammatory response producing redness, pain, and peeling, but there are additional sun-triggered rash conditions that are frequently confused with or occur alongside sunburn. Polymorphic light eruption (PLE), the most common photodermatosis, causes itchy papules, vesicles, or plaques on sun-exposed skin within hours of UV exposure — it affects 10–15% of the population, particularly fair-skinned women. Solar urticaria causes hives within minutes of sun exposure. Photocontact dermatitis occurs when sunscreen chemicals, NSAIDs, or plant compounds react with UV light on the skin. Photosensitive drug reactions produce a sunburn-like or morbilliform rash on sun-exposed skin from medications including tetracyclines, thiazide diuretics, fluoroquinolones, and NSAIDs. Heat rash (miliaria) from sweating in the sun is also common and adds to the rash burden. Understanding which sun-related rash you have determines the correct prevention and treatment strategy.
Quick Medical Summary
Polymorphic Light Eruption: The Most Common Sun Rash
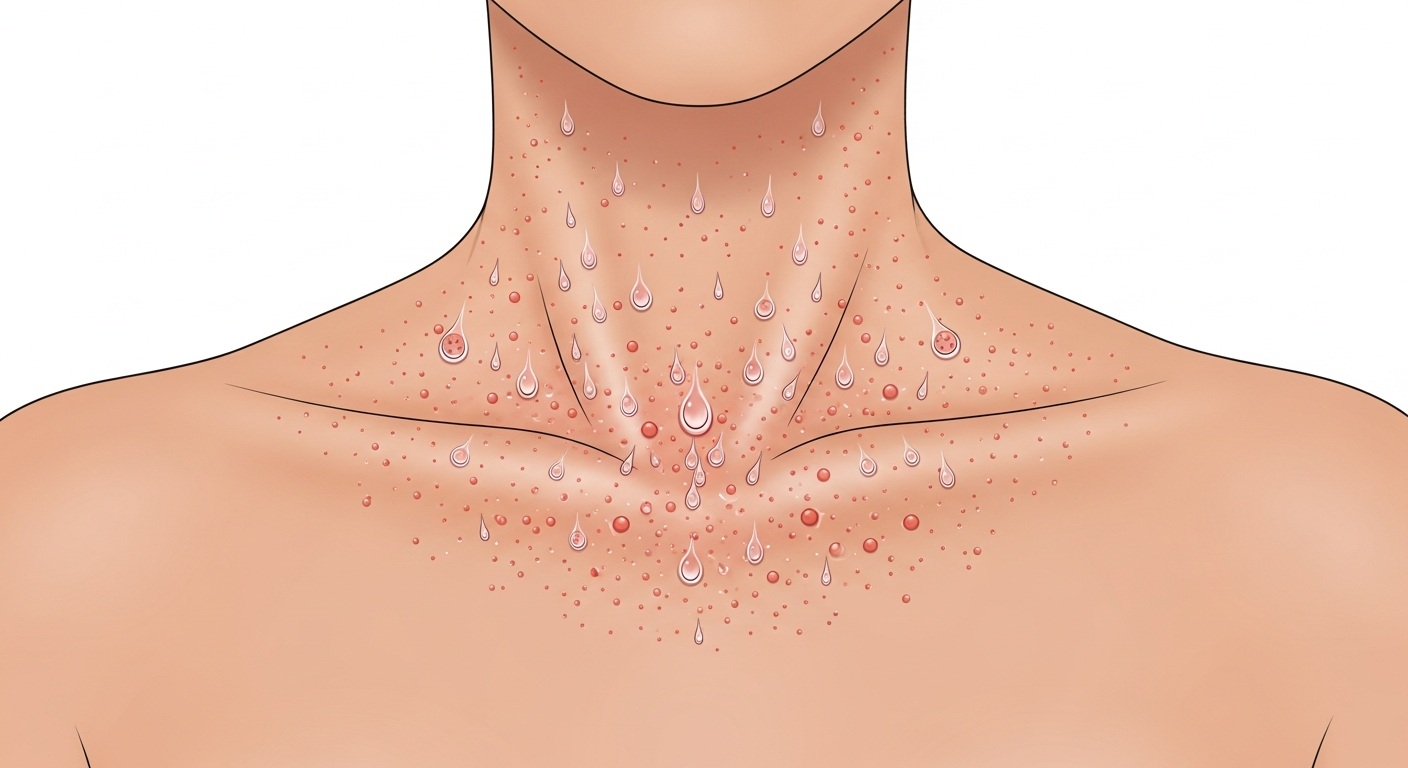
Polymorphic light eruption (PLE) affects 10–15% of fair-skinned populations — predominantly women — and is characterized by an itchy rash on sun-exposed skin that appears within hours (typically 30 minutes to 24 hours) of UV exposure. The 'polymorphic' name reflects the variety of lesion types: papules (most common), vesicles, plaques, or erythema multiforme-like target lesions — but importantly, each individual patient tends to develop the same lesion type each time they react. PLE most commonly affects the décolletage (upper chest), outer forearms, and tops of the feet — areas that receive intense UV exposure after winter, when the skin's protective mechanisms have not yet adapted. It typically starts in spring and early summer (when UV intensity suddenly increases after winter), and many patients find that continued daily sun exposure leads to gradual tolerance — 'hardening' — so the rash improves through the summer. This explains why PLE is worst during initial sun exposure (a vacation abroad, first hot days of spring) rather than mid-summer for regular outdoor workers. Prevention: gradually building sun exposure in spring (desensitization), applying high-SPF broad-spectrum sunscreen (UVA and UVB) before going out, wearing UV-protective clothing, and avoiding peak UV hours (10am–4pm). Persistent or severe PLE may respond to narrowband UVB desensitization therapy administered in a dermatology department.
Photocontact Dermatitis and Solar Urticaria
Photocontact dermatitis requires both a photosensitizing substance on the skin AND UV light simultaneously. Phototoxic reactions (non-immune, dose-dependent) occur in anyone exposed to sufficient chemical plus UV — the most dramatic examples are psoralen-containing plants (giant hogweed, parsnip, celery, lime) causing intense, blistering, burning rash within 24 hours of skin contact and sun exposure. This is called phytophotodermatitis — the rash is shaped exactly where the plant juice contacted the skin (often irregular, drip-like streaks or hand-shaped patterns). Photoallergic reactions require prior immune sensitization and affect only sensitized individuals — common culprits include sunscreen ingredients (benzophenone-3/oxybenzone, now declining due to reformulation), topical NSAIDs (ketoprofen gel — common in Europe), and fragrances. The photoallergic rash appears in a sun-exposed distribution but may spread beyond strictly sun-exposed areas as the immune reaction amplifies. Patch testing under UV (photopatch testing) identifies the specific photoallergen. Solar urticaria causes immediate hives within 5–10 minutes of sun exposure on uncovered skin — the wheals fade within 30–60 minutes of going indoors. It is a rare condition where IgE-mediated mast cell activation is triggered by specific UV wavelengths. Severe solar urticaria can cause anaphylaxis. Treatment includes high-SPF sunscreen, antihistamines before sun exposure, and in severe cases, omalizumab or PUVA desensitization.
Photosensitizing Medications and Sun-Related Rash Prevention
Multiple commonly prescribed medications make the skin hypersensitive to UV light, producing sunburn-like or morbilliform rashes on sun-exposed skin in a sun-exposed distribution. Tetracycline antibiotics (doxycycline, minocycline) — particularly relevant because they are used for rosacea, acne, and Lyme disease, often in summer — cause phototoxic reactions: exaggerated sunburn on minimal UV exposure. Thiazide diuretics (hydrochlorothiazide) — widely prescribed for hypertension — are photosensitizing and associated with increased risk of squamous cell carcinoma with long-term use. Fluoroquinolone antibiotics (ciprofloxacin), sulfonamides, and certain antifungals (voriconazole) are photosensitizers. NSAIDs (naproxen, piroxicam), phenothiazines (promethazine), and amiodarone cause both phototoxic and photoallergic reactions. If you start a new medication and develop an unusual sunburn-like rash on sun-exposed skin, report it to your prescribing doctor. Photoprotection while on photosensitizing drugs: SPF 50+ broad-spectrum sunscreen, UV-protective clothing (UPF 50), wide-brimmed hat, and avoidance of peak sun hours. For all sun-related rashes, broad-spectrum sunscreen with both UVA and UVB protection (PA+++ or 5-star UVA rating + SPF 50+) is the cornerstone of prevention.
Key Symptoms
- Itchy papules or vesicles on chest, forearms, and feet after spring/summer sun (PLE)
- Linear, streak-shaped blisters after plant juice + sun exposure (phytophotodermatitis)
- Hives appearing within 5–10 minutes of sun exposure (solar urticaria)
- Sunburn-like rash after minimal sun exposure while on antibiotics or diuretics
- Rash in sun-exposed distribution from sunscreen ingredients (photoallergic dermatitis)
- Exaggerated blistering sunburn from doxycycline or ciprofloxacin
Treatment Options
- PLE: high-SPF broad-spectrum sunscreen; gradual sun exposure in spring for hardening
- Phytophotodermatitis: wash plant juice off immediately; cool compresses; hydrocortisone cream
- Solar urticaria: pre-sun antihistamines; sunscreen; specialist review for severe cases
- Drug-induced photosensitivity: discuss medication with prescriber; maximize photoprotection
- Photoallergic dermatitis: photopatch testing to identify allergen; permanent avoidance
- General: SPF 50+ broad-spectrum sunscreen daily; UV-protective clothing; avoid 10am–4pm sun
When to See a Doctor Immediately
- Difficulty breathing or swallowing
- Swelling of the face, lips, or tongue
- High fever or severe chills
- Rapid spreading over a large body surface area
- Extreme pain, dizziness, or confusion
Frequently Asked Questions
Disclaimer
The medical information provided in this article is for educational purposes only and should not replace professional medical advice, diagnosis, or treatment. Always consult with a board-certified dermatologist or primary care physician regarding any severe or persistent skin conditions.