Can Heat Cause a Rash?
Medically Reviewed By
Dr. Marcus Chen, FAAD
Last Updated
November 12, 2025
Yes — heat causes several distinct types of skin rash through different mechanisms. Heat rash (miliaria) occurs when excessive sweating blocks sweat ducts, causing sweat to leak into surrounding skin and trigger inflammation — producing tiny red prickly bumps in skin folds and on the back, chest, and neck. Cholinergic urticaria is triggered by any activity that raises core body temperature — exercise, hot baths, spicy food, or emotional stress — producing distinctive tiny (1–3mm), intensely itchy wheals surrounded by a large red flare, within minutes of the temperature trigger. Rosacea — a chronic facial vascular condition — flares with heat exposure, producing flushing, persistent redness, and papules. Contact urticaria from heat (heat urticaria) is rare — localized hives appearing at the exact site of heat contact. Erythema ab igne — a permanent lacy purplish-brown skin discoloration — develops from chronic repeated heat exposure (e.g., using a heating pad or laptop on bare skin). Different heat rashes require entirely different treatments.
Quick Medical Summary
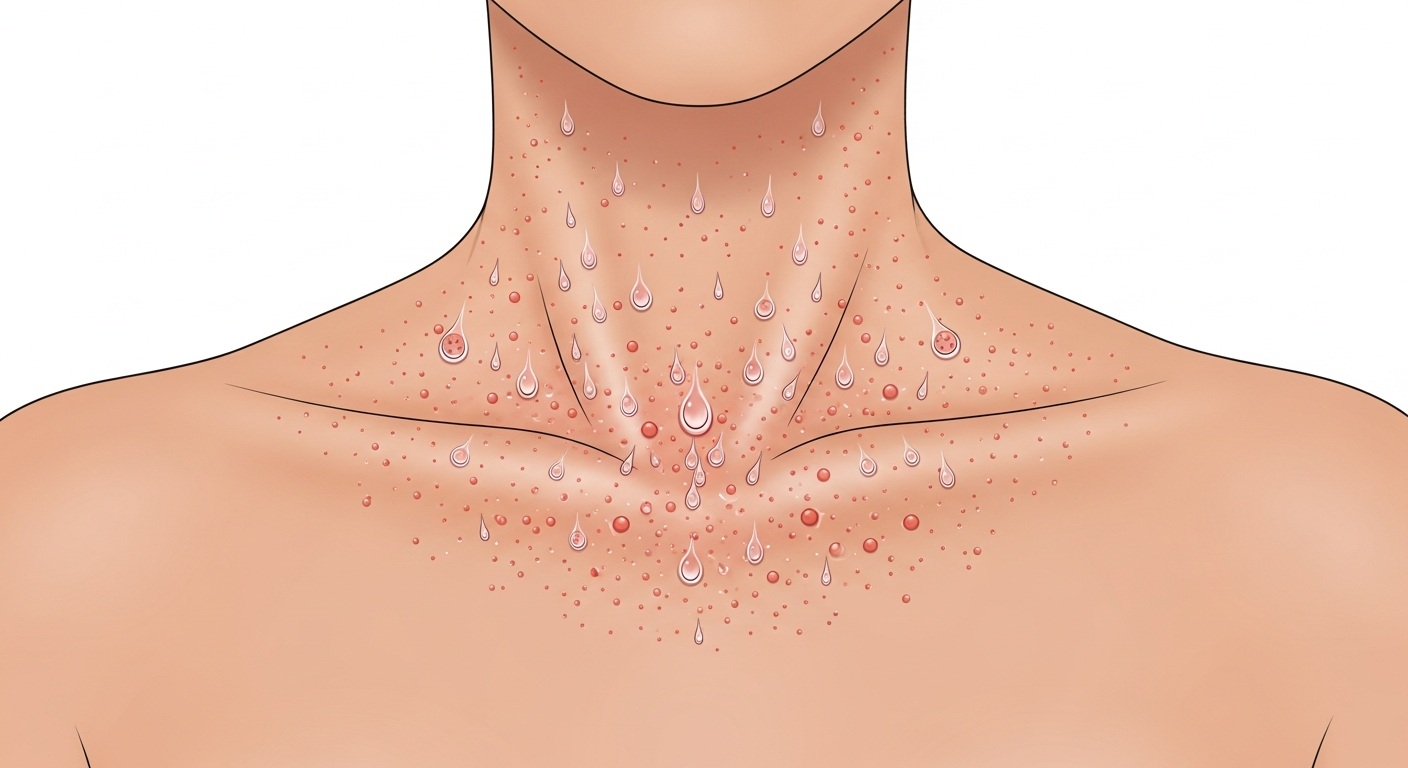
Heat Rash (Miliaria): Blocked Sweat Glands
Miliaria (heat rash, prickly heat) is the most common heat-related skin condition worldwide. It results from obstruction of eccrine sweat ducts at different depths within the skin, causing sweat to leak into surrounding tissue and trigger an inflammatory response. Three forms exist by depth of obstruction: miliaria crystallina (most superficial) — clear, thin-walled vesicles on the skin surface that rupture easily; not itchy, seen in newborns and in patients sweating heavily after fever. Miliaria rubra (heat rash, prickly heat) — the most common form — tiny red papules and vesicles in skin folds (neck, armpits, groin, under the breasts, on the back and chest), with intense prickling or burning sensation. Miliaria profunda — deeper sweat gland blockage — firm, flesh-colored papules that are less itchy but can impair sweating function significantly; occurs after repeated bouts of miliaria rubra. Risk factors: heat, humidity, tight synthetic clothing, obesity (creating multiple skin folds), bed rest (particularly in hospital patients), neonates (sweat gland immaturity), and certain medications (bethanechol, neostigmine). Treatment: move to cool environment; remove occlusive clothing; cool shower; calamine lotion; hydrocortisone 1% for inflammation. Miliaria profunda may require dermatology referral if extensive.
Cholinergic Urticaria: Temperature-Sensitive Hives
Cholinergic urticaria is a distinctive and often misunderstood heat-triggered hive condition affecting approximately 5–7% of young adults. The trigger is any elevation of core body temperature — exercise (running, weightlifting), hot baths or showers, spicy food, sauna, fever, or emotional stress causing sweating. The rash appears within 5–15 minutes of the trigger: tiny (1–3mm) rounded wheals, far smaller than typical urticaria, surrounded by a large red flare. The rash is intensely itchy, burning, and may be accompanied by a systemic flushing sensation. It typically resolves within 30–60 minutes of cooling down. Severe cases may progress to anaphylaxis — throat swelling and breathing difficulty — though this is uncommon. Diagnosis is confirmed by an exercise challenge or hot bath provocation test under medical supervision. Treatment: oral non-sedating antihistamines (cetirizine is most effective) taken 1 hour before anticipated triggers; dose-escalating from 10mg to higher doses if needed. For refractory cases, omalizumab (anti-IgE biologic) is dramatically effective. Patients should exercise in cool environments, avoid hot baths, and carry antihistamines. Desensitization therapy — regular exercise to maintain raised core temperature — can induce tolerance in some patients.
Rosacea Flushing, Erythema ab Igne, and Other Heat Rashes
Rosacea is a chronic inflammatory condition of facial blood vessels and sebaceous glands. Heat is one of its primary triggers — exposure to sun, hot drinks, alcohol, spicy food, exercise, and hot environments causes episodic flushing (intense redness and warmth of the face) that, over years, becomes persistent background facial redness. The flushing is caused by heat-induced vasodilation of facial blood vessels, which in rosacea are chronically inflamed and hyper-responsive. Management: avoidance of heat triggers; topical brimonidine or oxymetazoline gel to constrict facial vessels; oral tetracyclines for papular/pustular component; laser or intense pulsed light (IPL) for telangiectasia. Erythema ab igne (toasted skin syndrome) is a permanent skin change caused by chronic repeated moderate heat exposure — typically from heating pads, hot water bottles, electric blankets, or laptops resting on bare skin. The skin develops a lacy, net-like pattern of reddish-brown or purple discoloration (livedo-like) in the area of chronic heat contact. It is benign and does not require treatment, but the discoloration may be permanent. Avoid the heat source. Rarely, chronic erythema ab igne can predispose to squamous cell carcinoma in the affected area after decades. Exercise-induced anaphylaxis — different from cholinergic urticaria — causes widespread urticaria, angioedema, and anaphylaxis during or immediately after exercise, sometimes requiring food ingestion as a cofactor (food-dependent exercise-induced anaphylaxis).
Key Symptoms
- Tiny red prickly bumps in skin folds during hot weather (heat rash/miliaria)
- Small intense wheals with large flare within minutes of exercise or hot bath (cholinergic urticaria)
- Facial flushing and persistent redness with heat, alcohol, or spice triggers (rosacea)
- Lacy purple-brown permanent skin pattern from chronic heat exposure (erythema ab igne)
- Localized hives exactly where hot object contacted skin (contact heat urticaria)
- Exercise-triggered widespread hives with angioedema (exercise-induced anaphylaxis)
Treatment Options
- Heat rash: cool environment, cool shower, calamine lotion, loose cotton clothing
- Cholinergic urticaria: cetirizine 1 hour before triggers; omalizumab for severe cases
- Rosacea: heat trigger avoidance; topical brimonidine; oral doxycycline; IPL laser
- Erythema ab igne: remove heat source; discoloration may be permanent
- Exercise-induced anaphylaxis: carry epinephrine auto-injector; avoid cofactor foods before exercise
- Miliaria profunda (extensive): dermatology referral; consider systemic interventions
When to See a Doctor Immediately
- Difficulty breathing or swallowing
- Swelling of the face, lips, or tongue
- High fever or severe chills
- Rapid spreading over a large body surface area
- Extreme pain, dizziness, or confusion
Frequently Asked Questions
Disclaimer
The medical information provided in this article is for educational purposes only and should not replace professional medical advice, diagnosis, or treatment. Always consult with a board-certified dermatologist or primary care physician regarding any severe or persistent skin conditions.