Rash on Chest: Causes, Symptoms, and Treatment
Medically Reviewed By
Dr. Marcus Chen, FAAD
Last Updated
February 17, 2026
The chest is one of the most common locations for skin rash because it is the trunk — the starting point for many systemic rashes that begin centrally (viral exanthems, drug rashes, pityriasis rosea), a common site for sweat accumulation promoting heat rash and tinea versicolor, a sun-exposed area predisposing to polymorphic light eruption on the décolletage, and an area of frequent contact with jewelry, bra straps, and fabric dyes. The most important chest rash not to miss is shingles (herpes zoster) — a unilateral, dermatomal blistering rash preceded by burning pain that requires antiviral treatment within 72 hours of rash onset to prevent post-herpetic neuralgia. Beyond shingles, the key diagnostic distinction on the chest is between the trunk-centered, bilateral symmetrical rashes (pityriasis rosea, drug reactions, seborrheic dermatitis, viral exanthems) and the unilateral, dermatomal, pain-associated rash of shingles. This guide covers each major chest rash cause with identifying features, comparison table, and evidence-based treatment.
Quick Medical Summary
Most Common Causes of Chest Rash
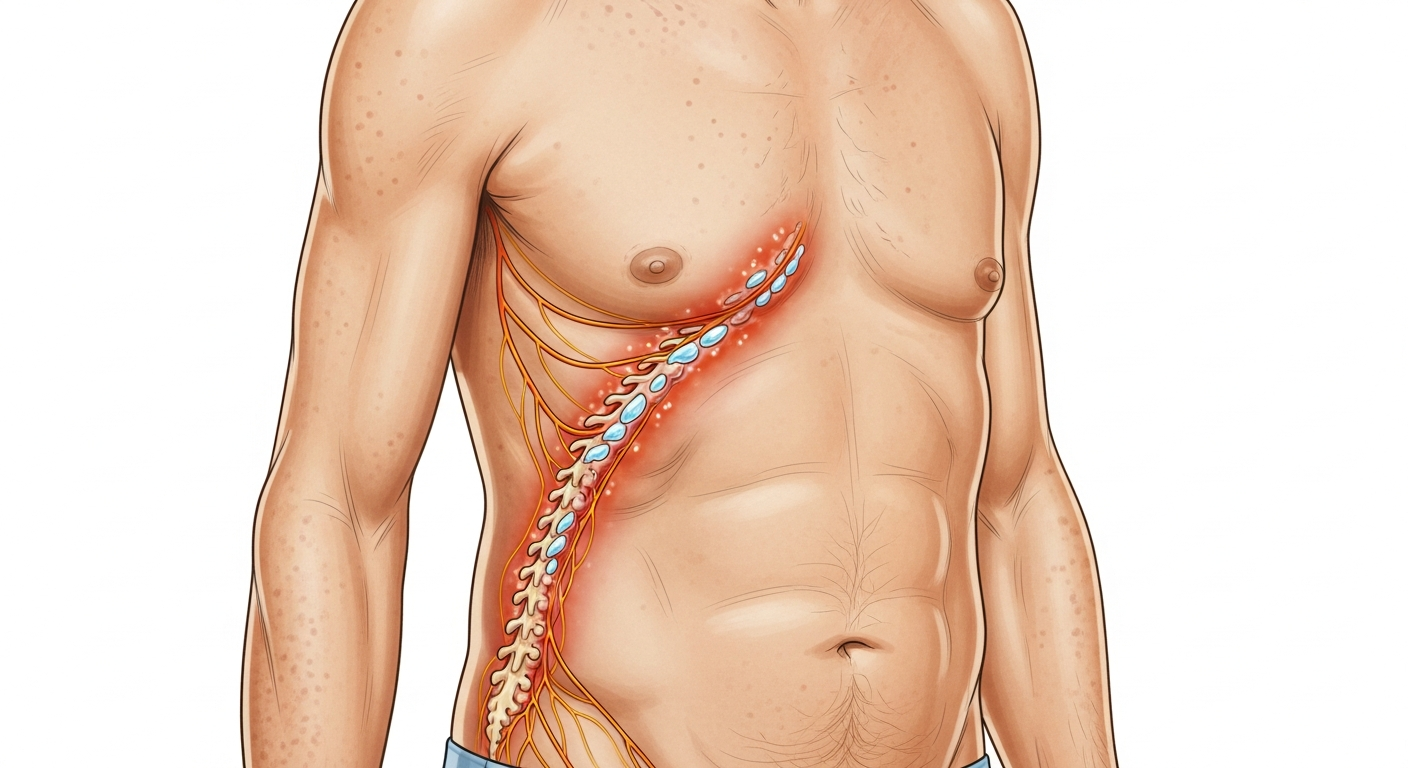
Shingles (herpes zoster) on the chest is caused by reactivation of the varicella-zoster virus (chickenpox) from the dorsal root ganglia along a thoracic dermatome — a band of skin innervated by a single nerve root on one side of the chest from the spine around to the midline. The cardinal distinguishing features: (1) it is strictly unilateral — never crossing the midline; (2) it is dermatomal — following the curved band of the nerve root; (3) burning, shooting, or aching pain precedes the rash by 1–3 days; (4) grouped vesicles on a red base appear in the dermatomal distribution and crust over 7–10 days. Start antiviral therapy (valaciclovir 1g three times daily for 7 days) within 72 hours of rash onset. Pityriasis rosea begins with a single 'herald patch' — a solitary, oval, salmon-pink patch with a collarette of fine scale, typically 2–5cm in diameter, appearing on the chest or upper back 1–2 weeks before the full eruption. Subsequently, numerous smaller oval patches spread across the trunk in a 'Christmas tree' pattern — oriented along skin tension lines (Langer's lines), fanning diagonally outward from the spine across the back, and running in the rib direction on the chest. It is mildly itchy and self-limiting, resolving in 6–12 weeks. Seborrheic dermatitis on the chest produces yellowish-white, greasy scale on the central upper chest (the sternal area between the pectorals and below the clavicle), mirroring its scalp and facial distribution. It responds to antifungal wash (ketoconazole shampoo used as a body wash). Tinea versicolor — a superficial yeast (Malassezia) infection — produces hypo- or hyperpigmented oval patches on the chest, upper back, and shoulders, particularly visible in tanned skin where the affected areas fail to tan, or in lighter skin where they produce faintly pink or tan discolored patches.
Symptom Breakdown and Identifying Your Chest Rash
Timing and onset pattern are the most useful initial clues for chest rash. A rash that began with severe burning pain on one side of the chest 1–3 days before appearing is shingles until proven otherwise — do not wait for the rash to appear fully if this pre-rash pain pattern is described. A single large oval patch that preceded a more widespread rash by 1–2 weeks is the herald patch of pityriasis rosea. A rash appearing 7–14 days after starting a new medication (antibiotics, NSAIDs, anticonvulsants) that began on the trunk and is spreading symmetrically suggests a morbilliform drug eruption — stop the medication and seek medical evaluation if spreading continues. Pattern and distribution are the next key diagnostic tool. Unilateral band: shingles. Christmas-tree bilateral: pityriasis rosea. Central sternal with yellowish scale: seborrheic dermatitis. Discrete pale or tan patches failing to tan uniformly: tinea versicolor. Widespread pink spots starting on trunk and spreading to limbs with fever: viral exanthem. Under breasts, in skin folds: heat rash or candidal intertrigo. Inframammary fold with raw, moist, bright-red appearance and satellite pustules: Candida (yeast rash). Multiple comedones, papules, and pustules across the chest and upper back: truncal acne. Oval scaly patches along rib lines: pityriasis rosea. Acne: small comedones (blackheads, whiteheads), papules, and pustules particularly on the upper chest, stimulated by sweat, friction from sports bras, and certain cosmetics (pomade acne).
When to Worry: Red Flags for Chest Rash
Unilateral chest rash with severe preceding pain must be treated as shingles and antivirals started within 72 hours — delay increases the risk of post-herpetic neuralgia, a chronic and debilitating nerve pain condition lasting months to years. Any non-blanching rash across the chest accompanied by high fever, neck stiffness, or severe headache may indicate meningococcal septicemia — press a glass against the rash; if spots remain visible, call emergency services immediately. A blistering, painful rash spreading rapidly across the chest with mucosal involvement (mouth sores, eye redness, genital blistering) starting 7–14 days after starting a new drug is Stevens-Johnson Syndrome — stop all suspect medications and go to the emergency department. This is a medical emergency with significant mortality. Drug rash evolving from flat pink spots to blistering or purpuric lesions, accompanied by facial swelling, lymph node enlargement, or organ inflammation (elevated liver enzymes) may represent Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) — another medical emergency. Chest rash with joint pain, fatigue, oral ulcers, and butterfly rash on the face suggests systemic lupus erythematosus — requires lupus serology (ANA, anti-dsDNA) and rheumatology referral. Persistent, non-healing, scaly, or bleeding patches on sun-exposed décolletage in older adults may represent actinic keratoses (pre-cancerous) or squamous cell carcinoma — dermatology referral for examination and possible biopsy.
Treatment Overview for Chest Rash
Shingles: valaciclovir 1g three times daily for 7 days — start within 72 hours of rash onset. Pain management: NSAIDs, paracetamol for mild pain; amitriptyline, gabapentin, or pregabalin for neuropathic post-herpetic neuralgia; topical lidocaine patch for localised neuralgia. Vaccination with Shingrix (recombinant zoster vaccine) is recommended for all adults over 50 and immunocompromised individuals over 18 to prevent shingles. Pityriasis rosea: no specific treatment is needed — it resolves spontaneously in 6–12 weeks. Antihistamines for itch. Moderate UVB light exposure or narrowband UVB in clinic speeds resolution. Aciclovir (oral) may shorten the course if herpes virus trigger is suspected. Seborrheic dermatitis on the chest: apply ketoconazole 2% shampoo to the chest, leave for 5 minutes, then rinse, 2–3 times per week during active phase, then weekly for maintenance. Selenium sulfide shampoo is an alternative. Tinea versicolor: selenium sulfide 2.5% shampoo (Selsun) applied to the chest and left for 10 minutes before rinsing, three nights weekly for 4 weeks; or ketoconazole shampoo in the same manner; or a single oral dose of fluconazole 400mg or itraconazole. Note that pigmentary changes (pale or darker patches) may take months to normalize even after the infection is cleared. Heat rash and inframammary rash: cool environment, loose clothing, calamine lotion; keep the inframammary fold dry using a folded cotton cloth as an absorbent barrier; topical clotrimazole cream for candidal inframammary rash. Acne on chest: benzoyl peroxide body wash (5–10%); topical retinoid (adapalene, tretinoin); topical clindamycin; oral antibiotics (doxycycline) for inflammatory acne; isotretinoin for severe disease.
Key Symptoms
- Burning pain on one side of chest 1–3 days before rash (pre-shingles neuralgia)
- Unilateral blistering band across one side of chest following nerve line (shingles)
- Single large oval patch followed by Christmas-tree distribution (pityriasis rosea)
- Yellowish scale on central sternal area (seborrheic dermatitis)
- Pale or tan patches not tanning uniformly on chest/back (tinea versicolor)
- Tiny red prickly bumps under the breasts or in skin folds (heat rash)
- Bright red rash with satellite pustules under breasts (candidal intertrigo)
- Widespread pink spots on trunk spreading to limbs with fever (viral/drug rash)
Treatment Options
- Shingles: valaciclovir 1g 3× daily for 7 days — start within 72 hours
- Pityriasis rosea: antihistamines; UVB light; self-resolves in 6–12 weeks
- Seborrheic dermatitis: ketoconazole shampoo 2–3× weekly on chest
- Tinea versicolor: selenium sulfide or ketoconazole shampoo for 4 weeks
- Candidal intertrigo: topical clotrimazole; keep area dry; cotton barrier
- Heat rash: cool environment; calamine lotion; loose breathable clothing
- Truncal acne: benzoyl peroxide wash; topical retinoid; doxycycline for inflammatory
- Drug rash with mucosal involvement: stop medication; emergency evaluation
| Condition | Laterality | Key Distinguishing Feature | Requires Urgent Care? |
|---|---|---|---|
| Shingles (Herpes Zoster) | Strictly unilateral | Preceded by burning pain; blistering dermatomal band | Yes — antiviral within 72h |
| Pityriasis Rosea | Bilateral, symmetric | Herald patch first; Christmas-tree pattern | No — self-limiting |
| Seborrheic Dermatitis | Central, bilateral | Yellowish-greasy scale, sternal area | No — antifungal wash |
| Tinea Versicolor | Bilateral (back > chest) | Hypo/hyperpigmented patches, fails to tan | No — antifungal treatment |
| Viral/Drug Rash | Bilateral, from trunk out | Appeared with fever or new drug | Monitor — stop drug; see doctor |
| SJS/TEN | Bilateral, spreading rapidly | Blistering with mucosal involvement | Emergency — go to ER now |
Diagnose and Treat Your Rash
When to See a Doctor Immediately
- Difficulty breathing or swallowing
- Swelling of the face, lips, or tongue
- High fever or severe chills
- Rapid spreading over a large body surface area
- Extreme pain, dizziness, or confusion
Frequently Asked Questions
Disclaimer
The medical information provided in this article is for educational purposes only and should not replace professional medical advice, diagnosis, or treatment. Always consult with a board-certified dermatologist or primary care physician regarding any severe or persistent skin conditions.