Elderly Rashes: Common Skin Conditions in Adults Over 60
Medically Reviewed By
Dr. Marcus Chen, FAAD
Last Updated
November 20, 2025
Elderly skin undergoes profound structural and functional changes that directly drive the characteristic rash patterns of old age. After age 60, the epidermis (outer skin layer) thins and loses its ability to maintain adequate moisture, producing the dry, fragile skin that underlies the most prevalent elderly skin condition — asteatotic eczema (eczema craquelé). The dermis loses collagen, elastin, and ground substance, reducing skin strength and elasticity. Subcutaneous fat diminishes, reducing cushioning and insulation. The skin microvasculature becomes more fragile, producing the characteristic gravitational purpura (non-blanching red-brown spots) of elderly legs from minimal trauma. Immune senescence — the age-related decline in immune function — dramatically increases the risk and severity of shingles (herpes zoster), reduces vaccine responses, and allows malignant transformation of skin cells to proceed unchecked, raising skin cancer risk substantially. The number of medications typically increases with age, dramatically raising the probability of drug-induced rashes. Bullous pemphigoid — a blistering autoimmune skin disease — is almost exclusively an elderly condition, with incidence rising steeply from age 70 onward. This comprehensive guide covers the most clinically important rashes in adults over 60, their causes, distinguishing features, prevention strategies, and treatment — with reference to the specialist silo pages for diagnosis and symptom assessment.
Quick Medical Summary
Asteatotic Eczema, Drug Rashes, and Gravitational Purpura
Asteatotic eczema (eczema craquelé — 'crazy paving' eczema) is the most common rash in elderly adults, caused by the combined effects of reduced sebum production (the skin's natural moisturizing mechanism), lower epidermal barrier function, environmental dryness (central heating, air conditioning), hot baths, and harsh soaps. It appears as a dry, cracked, scaling rash with a distinctive 'crazy paving' or 'cracked china' appearance — the skin surface resembles dried mud or cracked porcelain, typically on the lower legs, arms, and trunk. It is intensely itchy and often misdiagnosed as scabies (though scabies in elderly patients is also common and underdiagnosed). Treatment: use a soap substitute or emulsifying ointment for washing (never regular soap, which strips remaining skin lipids); apply thick emollient immediately after bathing and throughout the day; use a bedroom humidifier; topical corticosteroids for actively inflamed areas. Drug-induced rashes increase in frequency with age because elderly patients typically take more medications (polypharmacy), are more likely to receive new prescriptions, and have slower drug metabolism that allows drugs to accumulate. Morbilliform (measles-like) drug eruptions beginning 7–14 days after starting a new medication are the most common drug rash type and can occur with almost any medication. NSAIDs, antibiotics, diuretics, ACE inhibitors, and allopurinol are particularly common causes. Gravitational purpura (senile purpura) — now preferably called actinic purpura — produces large, dark-red to purple, irregular, non-painful, non-blanching patches on sun-damaged forearms and legs of elderly individuals from trivially minor trauma — the skin and subcutaneous tissue no longer provide adequate protection for the fragile capillaries beneath. It is benign but can look alarming and be confused with more serious causes of purpura.
Shingles and Bullous Pemphigoid in Elderly Patients
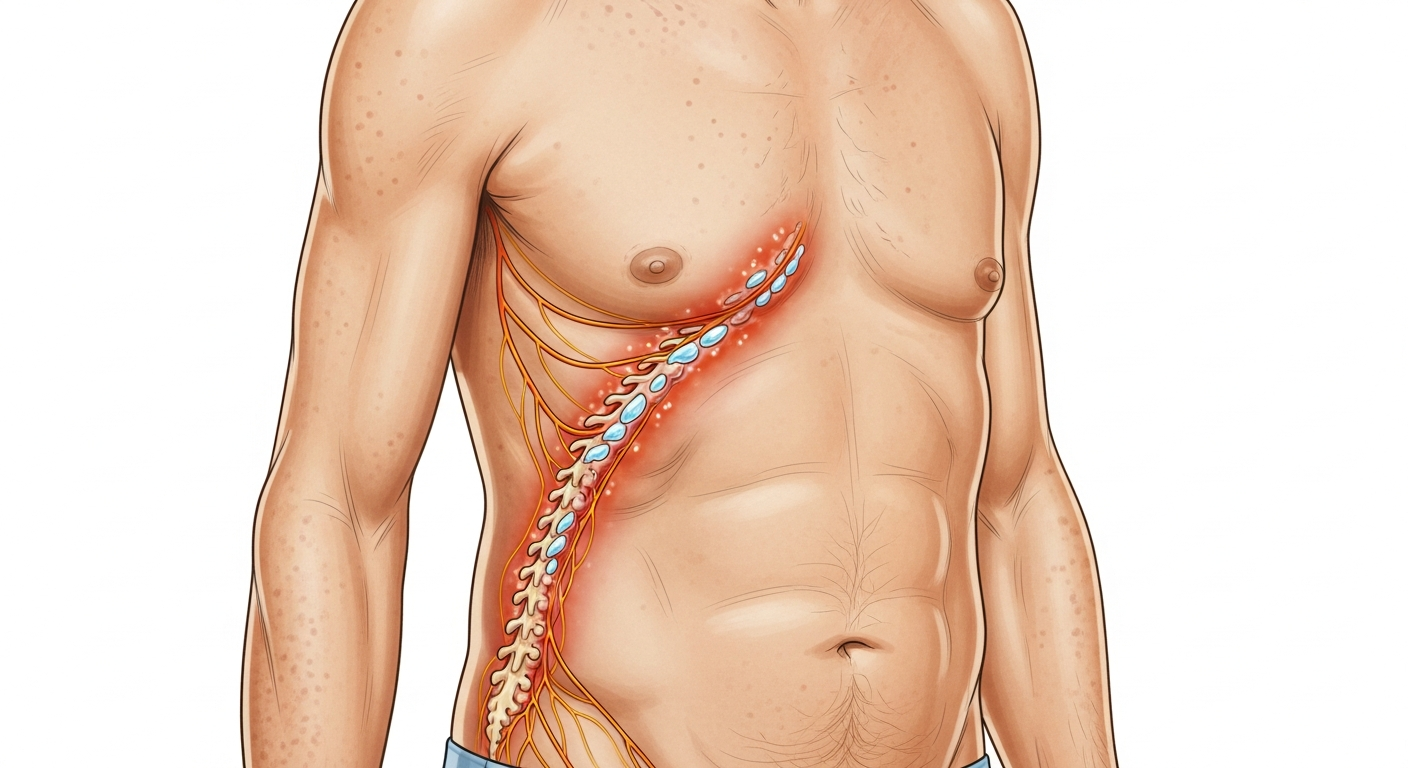
Shingles (herpes zoster) risk rises sharply from age 50 onward, with the highest incidence in adults over 70. This age-related increase reflects immune senescence — the decline in varicella-zoster-specific T-cell immunity that normally keeps the latent virus suppressed in the dorsal root ganglia. Shingles in elderly patients is significantly more severe than in younger adults: the acute rash is more painful, takes longer to heal, and the risk of post-herpetic neuralgia (PHN) — chronic neuropathic pain lasting months to years in the dermatomal distribution of the rash — rises dramatically with age (under 60: 5% risk of PHN; over 70: 30% risk; over 80: 50% risk). Shingles in the ophthalmic branch of the trigeminal nerve (herpes zoster ophthalmicus — forehead, scalp, nose tip) can cause permanent vision loss and requires same-day ophthalmology evaluation alongside antiviral treatment. Antiviral therapy (valaciclovir 1g three times daily for 7 days) within 72 hours of rash onset significantly reduces the duration and severity of acute shingles and the probability of PHN. The recombinant zoster vaccine (Shingrix, given in two doses) provides approximately 90% protection against shingles and more than 85% protection against PHN in adults over 50. Bullous pemphigoid (BP) is an autoimmune blistering condition caused by autoantibodies against two structural proteins in the dermo-epidermal junction (BP180 and BP230), causing detachment of the epidermis from the dermis and producing large, tense blisters on an erythematous base on the trunk and limbs. It is almost exclusively an elderly disease — incidence rises 50-fold from age 60 to age 90. The blisters are preceded by an intensely itchy urticarial phase, often misdiagnosed as chronic urticaria. Diagnosis requires skin biopsy with direct immunofluorescence. Treatment: potent topical clobetasol propionate 0.05% (first-line for limited disease); oral prednisolone with steroid-sparing agents (doxycycline, nicotinamide, azathioprine) for moderate-to-severe disease.
Age-Related Immune Changes and Skin Cancer Risk in Elderly Patients
Immune senescence — the age-related quantitative and qualitative decline in immune function — is a central factor in the rash and skin disease patterns of elderly individuals. Naive T-cell production declines as the thymus involutes with age. Memory T-cell function becomes more variable and less regulated. Natural killer (NK) cell activity decreases. The inflammatory response is dysregulated — paradoxically, older adults often show systemic low-grade chronic inflammation (inflammaging) while simultaneously being less capable of mounting effective acute immune responses to new infections. The practical consequences for skin disease include: dramatically increased shingles risk (failed VZV immunity); higher susceptibility to severe scabies infestations (Norwegian/crusted scabies — a severe hyperinfestation occurring in immunocompromised and elderly individuals who cannot mount an adequate immune response to the mite); slower wound healing from reduced fibroblast activity and impaired neutrophil function; higher risk of secondary bacterial infection of skin lesions; and a substantially elevated skin cancer risk. UV damage accumulates throughout life — decades of UV exposure cause DNA mutations in keratinocytes (skin cells) that are normally identified and eliminated by immune surveillance. With age-related immune senescence, this surveillance function declines, allowing mutated cells to progress to actinic keratoses (pre-cancerous), squamous cell carcinoma, and basal cell carcinoma. Melanoma risk peaks in adults over 70. Annual full-body skin examination by a dermatologist is recommended for adults over 60 with significant sun exposure history, a history of skin cancer, or multiple actinic keratoses.
Prevention, Treatment, and When to Seek Medical Care for Elderly Rashes
Prevention is particularly high-yield in elderly patients, where rashes can be more severe and slower to heal. Shingrix vaccination (two doses, 2–6 months apart) is the single most important preventive measure against shingles and post-herpetic neuralgia in adults over 50 — discuss with your GP. Daily emollient application prevents asteatotic eczema — apply a thick fragrance-free emollient (Doublebase gel, E45, or Vaseline) to dry areas immediately after bathing with tepid water using soap substitutes. Annual skin review with a dermatologist identifies actinic keratoses (pre-cancerous sun damage) that can be treated prophylactically before progression to squamous cell carcinoma. SPF 50+ sunscreen on exposed areas daily reduces further UV damage accumulation. Review medications regularly — the Beers Criteria identifies medications particularly risky in the elderly, some of which cause skin reactions; discuss medication reviews with your GP or pharmacist. Seek emergency care for: blistering rash spreading rapidly with mucosal involvement (SJS/TEN — from a new drug), anaphylaxis, non-blanching rash with systemic toxicity, and suspected necrotizing fasciitis (extremely painful, rapidly spreading skin infection — higher risk in elderly diabetics). Seek urgent same-day care for: shingles rash on the face (ophthalmologic emergency if near the nose or eyes), rapidly spreading cellulitis with fever, new blistering rash in an elderly patient (may be bullous pemphigoid requiring biopsy). Routine evaluation within 1–2 weeks for: new rash after medication change, suspected scabies (elderly patients with unexplained widespread itch and rash in care home settings), changing skin lesions, and non-healing skin wounds. See the full symptoms guide for systematic assessment, and the diagnosis guide for clinical evaluation methods.
Key Symptoms
- Dry, cracked, 'crazy paving' skin on lower legs and arms (asteatotic eczema)
- Large dark-red/purple non-painful patches on forearms after minor knock (actinic purpura)
- Burning pain on one body side followed by blistering band (shingles — antiviral urgent)
- Large tense blisters on trunk/limbs preceded by intense itch (bullous pemphigoid)
- New widespread rash 7–14 days after starting a medication (drug rash)
- Intense generalized itch with subtle skin changes in care home setting (possible scabies)
- Rough, scaly, or non-healing patch on sun-exposed skin (actinic keratosis or skin cancer)
- Non-blanching rash with systemic symptoms (emergency at any age)
Treatment Options
- Asteatotic eczema: soap substitute + thick emollient daily; bedroom humidifier
- Actinic purpura: reassurance; topical vitamin K cream; gentle skin protection
- Shingles: valaciclovir within 72h; gabapentin/pregabalin for PHN; Shingrix prevention
- Bullous pemphigoid: clobetasol 0.05% cream; oral prednisolone + steroid-sparing agents
- Drug rash: identify and stop causative drug; antihistamines; dermatology review
- Scabies in elderly: permethrin 5% or oral ivermectin; treat all care home contacts
- Actinic keratoses: cryotherapy; topical 5-FU or imiquimod; diclofenac gel
- Annual skin check: dermatologist review for sun-damaged or high-risk individuals
| Condition | Prevalence Over 70 | Hallmark Feature | Primary Treatment |
|---|---|---|---|
| Asteatotic Eczema | Very common (>30%) | Crazy-paving dry cracked skin, legs/arms | Daily emollient; soap substitute; mild steroid |
| Actinic Purpura | Very common | Large purple non-blanching patches, forearms | Reassurance; topical vitamin K; skin protection |
| Shingles | Rises steeply with age | Unilateral dermatomal blistering + severe pain | Valaciclovir within 72h; Shingrix vaccine |
| Bullous Pemphigoid | Almost exclusively elderly | Large tense blisters; preceding intense itch | Clobetasol 0.05%; oral immunosuppression |
| Drug Rash | Very common (polypharmacy) | Morbilliform rash 7–14 days after new drug | Stop causative drug; antihistamines; review |
| Skin Cancer | Highest risk over 60 | Non-healing, changing, or unusual lesion | Dermatology referral; biopsy; excision |
Further Reading by Age Group
When to See a Doctor Immediately
- Difficulty breathing or swallowing
- Swelling of the face, lips, or tongue
- High fever or severe chills
- Rapid spreading over a large body surface area
- Extreme pain, dizziness, or confusion
Frequently Asked Questions
Disclaimer
The medical information provided in this article is for educational purposes only and should not replace professional medical advice, diagnosis, or treatment. Always consult with a board-certified dermatologist or primary care physician regarding any severe or persistent skin conditions.